
ADHD in Adults
Author: Ulrich Brennecke
Review: Waldemar Zdero, M.A. in Psychology
ADHD does not, as was believed until the end of the last millennium,1 automatically end when a person reaches adulthood.
ADHD persists into adulthood in about two-thirds of the people with ADHD who were diagnosed as children. Many experience changes in their symptoms, while others may experience complete remission or remission with fluctuating phases. Up to 90% of people with ADHD still have residual symptoms or significant limitations in young adulthood compared to people without ADHD. Various reasons for the persistence of ADHD into adulthood are discussed, such as a low socioeconomic background, high stress levels during childhood, or late-onset trauma. One theory posits that ADHD is already present in childhood but is masked by coping mechanisms and only becomes apparent in adulthood. Late-onset ADHD—that is, when symptoms first appear (or at least become recognizable) in adulthood—is possible and can occur in up to 10% of ADHD cases, particularly among women.
The symptoms of ADHD differ in adults compared to children, with hyperactivity decreasing and inner restlessness, inattention, and organizational problems becoming more prominent.
ADHD can be diagnosed even in old age.23 The treatment of ADHD in adults often requires lower doses of stimulants than in children.
1. Persistence of ADHD into Adulthood
5% of all children have ADHD (and ADHD is suspected in another 5%). In the U.S., about 4.4% of all adults are affected by ADHD.45 Further studies can be found in Krause.6
One large study even found a higher prevalence of ADHD among adults (2.8%) than among children (2.2%).7 This could be consistent with the idea that the heritability of adult ADHD may be lower than that of childhood ADHD, meaning that environmental factors may play a greater role in the development of ADHD in adults than in children.8
1.1. Types of Survival and Their Prevalence
It is by far more the rule than the exception that ADHD present in childhood persists into adulthood.
The problem is that many longitudinal studies did not use the original diagnostic criteria during follow-up, but rather the DSM in effect at the time9, so that remission rates were influenced by changes in diagnostic criteria rather than solely by changes in symptoms.
1.1.1. ADHD in childhood can persist completely into adulthood
ADHD persists throughout a person’s life, possibly with changing symptoms, in
- about 66%1011
- 65.6%12
- 65% partial continuation13
- 50%14
- 35%1516
- 32%9
- 22%17
- 17.2% (based on the 1993 Pelotas Birth Cohort Study)18
- 15% full continuation13
- 4%19 (Old, significantly more restrictive ADHD criteria: DSM-III-R compared to DSM-II)
1.1.2. ADHD in childhood sometimes persists into adulthood
A reduction in ADHD, in the sense of a decrease in the number of symptoms, is referred to as partial remission. For most people with ADHD, for example, significant limitations remain in terms of educational and career achievements compared to people without the condition.
The percentage of people with ADHD in childhood who have partially persistent ADHD as adults has been estimated at
- 60%9
- 8% (Old, significantly narrower criteria: DSM-III, DSM-III-R compared to DSM-II)19
- 0.23% for a stable partial remission14
A study found that, among adults whose previous ADHD had gone into remission, only the following symptom groups
- Executive problems
- Behavioral problems
had been remitted, while
- Hyperactivity/restlessness
- Shortcomings in planning and organization
continued.12
1.1.3. Childhood ADHD with complete remission
Complete remission in adulthood, with no residual symptoms, was observed in
- 35%13
- 34.4%12
- 30%2014
- 10%20
- 8%9
- 5.7% over 21 years
- A study followed adults three times at intervals of 7 and 6 years, from an average age of 34 to an average age of 47. The study found a remission rate of 5.7%.21
- 0%22
Complete remission does not mean that the symptoms have disappeared entirely, but merely that they no longer meet the criteria required for a diagnosis. Educational deficits and lower academic performance persist.23
1.1.4. Fluctuating ADHD
Studies report a fluctuating course of ADHD, in which ADHD disappeared (went into remission) and reappeared (recurred) multiple times during development.231521242
ADHD persisted throughout life, with periods of remission and relapse, in
- 63.8% experienced alternating periods of remission and relapse during childhood and early adulthood1516
- This study was a follow-up to the MTA study and examined children with ADHD-C a total of 9 times from the start (mean age = 8.46) until the end of the follow-up study after 16 years (mean age = 25.12). In 63.8% of cases, ADHD disappeared intermittently (an average of 3.58 times) and then reappeared. The fluctuations within an individual averaged 6 to 7 symptoms between the peak and trough values, particularly during younger years. The severity of ADHD among these people with ADHD was generally moderate. The group with stable, persistent ADHD (10.8%) showed an early and persistent risk for mood disorders, substance use problems during adolescence and young adulthood, lower medication adherence, and a poorer response to treatment during childhood.
- Protective factors included
- in the recovery group: very low levels of parental psychopathology
- in the partial remission group: higher rates of comorbid anxiety
- 10% to 15% of cases of fluctuating ADHD14
A study reports on fluctuations in the severity of ADHD symptoms in children during the COVID-19 lockdown.25
ADHD symptoms identified in infants at 24 months of age showed moderate stability into preschool age, ranging from 56% to 60%.26
We believe that a certain proportion of fluctuating ADHD (but not all of it) is likely due to daily variations in symptom severity and the margin of diagnostic uncertainty when symptom severity is close to the diagnostic threshold. In addition, stress is likely to increase the severity of ADHD symptoms.
1.1.4.1. Are There Genetic Differences Between ADHD in Children and ADHD in Adults?
Longitudinal studies of twins suggest that genetic influences on ADHD are not static but change over the course of development. About half of the genetic variance in ADHD symptoms that occur during adolescence and early adulthood could be attributed to new, age-specific genetic factors.23272829
A GWAS found strong similarities in the genetic influences between childhood ADHD and adult ADHD.30
Another study found a broad overlap in the genetic architecture between childhood and adult traits for delay discounting and both positive and negative urgency, suggesting at least partial continuity in the underlying genetics across developmental stages. While a partial genetic overlap between children and adults was confirmed for some types of impulsivity, the remaining impulsivity indicators were not associated with their PGSs.31
One individual case involving a patient with clear-cut adult ADHD-C reported complete remission following a COVID-19 infection. After three-quarters of a year, the ADHD symptoms slowly returned. It is entirely conceivable that illnesses can alter the dopamine system. Just as certain viral illnesses can be a risk factor for ADHD because they can trigger an extracellular dopamine and norepinephrine deficiency in some brain regions, the reverse is also possible.
Although studies on fluctuating ADHD are rare, fluctuating ADHD could explain the well-known phenomenon in which many people with ADHD stop taking their medication—which they initially found very helpful and necessary—after a few years, only to resume taking it several years later.
1.2. Possible Reasons for ADHD Persisting into Adulthood
It is impossible to predict which people with ADHD will outgrow the condition in adulthood. Whether people with ADHD outgrow the condition by the age of 27 is independent of
- the severity of the disorder32
- the age at which ADHD first appeared32
- childhood IQ32
- Behavioral problems in childhood32
- the severity of ADHD-HI, ODD, or CD32
- the duration of stimulant treatment after adolescence32
There are various theories as to why ADHD that begins in childhood disappears in some adults but persists in others.
- Children with ADHD from low socioeconomic backgrounds benefited more from special educational support than children from higher socioeconomic backgrounds.33 In our view, this suggests that families with low socioeconomic status are less able to compensate for their children’s deficits. This is likely to apply to all mental health issues.
- A study of stress levels in children with ADHD found that high stress levels during childhood and adolescence were associated with severe ADHD-HI or ADHD-I course into adulthood, whereas children with low stress levels often exhibited remitting ADHD (all subtypes).34 A large cohort study in Sweden confirms this.35
- Another study found an up to 11.8-fold increase in the number of traumatic events among people with late-onset ADHD. Neurophysiologically, late-onset ADHD did not differ from ADHD in people with ADHD who had had the condition since childhood. However, the effects were significantly more severe. At the same time, one-third of people with late-onset ADHD were no longer diagnosed with ADHD after one year.36 The latter could also be an indication of a high rate of misdiagnosis.
- Puberty is accompanied by a marked change in dopaminergic innervation in the PFC. During this period, the PFC is particularly vulnerable to dopaminergic stimulation. This explains the behavior of adolescents, which oscillates between novelty-seeking and strong withdrawal. The high dopaminergic vulnerability during this developmental phase further explains the risks associated with alcohol and drug abuse or excessive media consumption. These can cause lasting disorders of the dopamine system, which increases the risk of impulsivity, addiction, or psychosis.37
Prolonged cortical maturation in the frontoparietal network has a beneficial effect on the brain’s ultimate performance, whereas accelerating this process—for example, through excessive dopaminergic stimulation—has an adverse effect.38 In both ADHD and giftedness, brain maturation is slowed.
See ⇒ Giftedness and ADHD In the section ⇒ Differential Diagnosis of ADHD in the chapter ⇒ Diagnosis
- Puberty is accompanied by a marked change in dopaminergic innervation in the PFC. During this period, the PFC is particularly vulnerable to dopaminergic stimulation. This explains the behavior of adolescents, which oscillates between novelty-seeking and strong withdrawal. The high dopaminergic vulnerability during this developmental phase further explains the risks associated with alcohol and drug abuse or excessive media consumption. These can cause lasting disorders of the dopamine system, which increases the risk of impulsivity, addiction, or psychosis.37
- Anxiety symptoms at age 15 make mental disorders in early adulthood significantly more likely:39
- Anxiety disorder: 4.9 times
- Depression: 4.8 times
- ADHD, ASD, or developmental disorder: 3.4 times
This could be further evidence that middle adolescence, along with early childhood, represents a second particularly vulnerable developmental window.
- One theory posits that brain functions mature later than usual. However, not every delay in brain maturation is necessarily a sign of ADHD. In gifted individuals, there is a delay in the development of the cortex that corresponds exactly to the delay in the emergence of the first peak in cortical thickness seen in ADHD.
⇒ ADHD and Giftedness. - Another theory suggests that certain regions of the brain take on compensatory functions, thereby correcting the child’s ADHD deficits.40
- Another model assumes that certain ADHD deficits in children persist throughout their lives.40
- A study of adults with persistent ADHD found an imbalance between the connections within the brain’s default-mode network, on the one hand, and those between the default-mode network and the areas that support attention and cognitive control, on the other. These differences were not present in adults whose ADHD had gone into remission.4142
- A comparison of adolescents with partial remission and those without remission revealed significantly lower activation of the vlPFC in the partial remission group. This improvement in vlPFC efficiency correlated with performance on a Go/No-Go task and fell between the ADHD group and normal controls.43
- A genetic analysis study identified four genome-wide significant loci for childhood ADHD and one for late-onset ADHD. In cases of persistent ADHD, elevated polygenic risk scores for ADHD (ADHD-PRS) were observed. Childhood ADHD showed greater genetic overlap with hyperactivity and autism, as well as the highest burden of rare protein-truncating variants in evolutionarily conserved genes. Late-onset ADHD, in contrast, showed greater genetic overlap with depression and no increased burden of rare protein-truncating variants.11
In adults with persistent ADHD, a thinner cortex was associated with more severe symptoms.44
2. Late-Onset ADHD
The term “late-onset” is used in English-language professional literature to refer to a later onset of ADHD that was only mild in childhood.
The vast majority of the literature uses the term “late-onset” to refer to a late initial diagnosis (in adulthood) that was not present during previous evaluations between the ages of 7 and 17 (DSM-IV) or 12 and 17 (DSM-5), without distinguishing whether or not individual symptoms were present during the first 6 or 11 years.
As we understand it, this conflicts with the classification systems of the DSM and ICD, for which the timing of the diagnosis is completely irrelevant, as long as several (= at least 2 of the 18 listed) symptoms had already appeared by age 6 (DSM-IV) or age 11 (DSM-5).
The term “late-onset” therefore does not describe anything particularly unusual, since the DSM and ICD naturally assume that the severity of symptoms can change with age.
Liu et al. coined the term “de novo late-onset” to describe full-blown ADHD that develops without multiple symptoms having been present during the first 6 or 11 years of life.45 They refer to a late diagnosis—one that, according to the DSM and ICD, was accompanied by some (but not enough for a diagnosis) symptoms in childhood—as “subthreshold late-onset ADHD” (subclinical late-onset ADHD). We consider the term “late-diagnosed ADHD”11 to be more appropriate.
However, some studies4623 also use the term “late-onset” to refer to “de novo late-onset,” which shows that the term is not only misleading to us (as discussed earlier).
2.1. Late Initial Diagnosis
Various long-term studies show that ADHD can be diagnosed for the first time even in adulthood. Depending on the study, this occurs in 0.4 to 10% of ADHD cases. For example, a study of young adults with ADHD found that only 12.6% had been diagnosed with ADHD during childhood.47
However, this already aligns with the definition in DSM-5 or ICD-11. Neither of these requires that ADHD be diagnosed for the first time only up to a certain age.
In cases of late initial diagnosis, a distinction must be made as to whether the symptoms were already severe enough during childhood that an ADHD diagnosis could have been made (missed diagnosis), whether the symptoms were not severe enough during childhood and only intensified later, or whether all ADHD symptoms first developed after the age thresholds specified by the DSM and ICD (de novo late-onset ADHD).
There is ongoing debate as to whether ADHD diagnosed later in life differs substantially from ADHD diagnosed in childhood. One study found that only 17.2% of children with ADHD were still diagnosed with ADHD as young adults, and only 12.6% of young adults had been diagnosed with ADHD during childhood.48 However, the DSM and ICD do not require a full-blown diagnosis in childhood, but rather only several (= at least 2) symptoms by age 11 (ICD-11 and DSM-5), which limits the significance of these figures. Other studies on the persistence of childhood ADHD into adulthood report rates of up to 66% (see above).
While ADHD in childhood showed a higher genetic overlap with hyperactivity and autism and the highest burden of rare protein-truncating variants in evolutionarily constrained genes, late-diagnosed ADHD was found to have a greater genetic overlap with depression and no increased burden of rare protein-truncating variants.11
2.1.1. Overlooked ADHD in Childhood: ADHD Diagnosed Late
Many people with ADHD who are diagnosed for the first time as adults already had enough and severe enough symptoms during childhood to have been diagnosed with ADHD back then.
In the last millennium, ADHD was known only to a few doctors and psychologists.
In this case, we propose the term “late-onset ADHD” or “late-recognized ADHD,” and in German, “spät erkanntes ADHD.”
2.1.2. Subclinical ADHD in Children: Subclinical Late-Onset ADHD
Adults who are diagnosed with ADHD for the first time do not necessarily have to have had diagnosable ADHD during childhood. It is sufficient that some (at least 2) symptoms had already appeared by the age of 6 (DSM-IV, ICD-10) or 11 (DSM-5, ICD-11). This is consistent with the standard definitions in the DSM and ICD.
To distinguish this case from those in which at most one or no ADHD symptoms were evident during childhood (de novo late-onset), the term “subthreshold late-onset ADHD,” coined by Liu et al., (subclinical late-onset ADHD) seems appropriate.
There is now clear evidence from extensive cohort studies in various countries that ADHD can also “first appear” in adulthood.49 One study showed that among children with ADHD, symptoms disappeared in adulthood for up to 95% of people with ADHD, while a significant proportion of adults with ADHD did not “have” a full-blown ADHD diagnosis as children.50
Population-based longitudinal studies show that, for a subset of people with ADHD, ADHD symptoms do not increase until after childhood, and they first meet the criteria for ADHD in late adolescence or early adulthood.4551 52 53 54 17 47 55 56 One study found that 45% of people with ADHD who were diagnosed as adults did not exhibit a full-blown ADHD diagnosis during childhood. These people showed lower levels of hyperactivity and impulsivity symptoms and had higher levels of education.57 We view both of these findings as indications of a higher likelihood of an overlooked diagnosis in childhood among individuals with good coping skills. In addition, greater resilience due to various protective factors is conceivable.
In a study of children aged 7 to 9 with subclinical psychiatric disorders, 37% had developed a full-blown form of the Disorder after 3 years.58
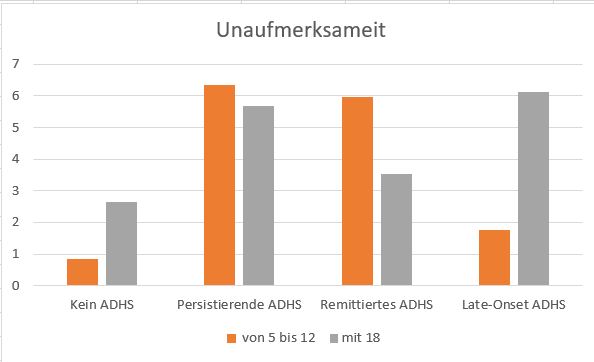
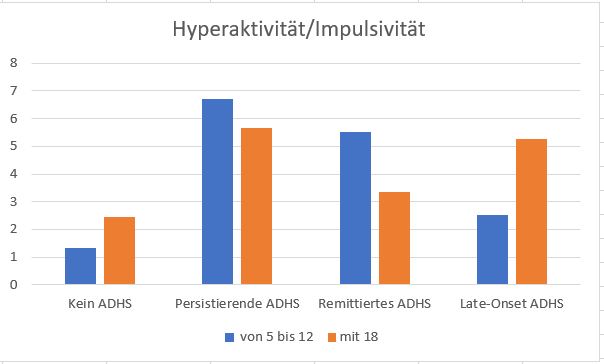
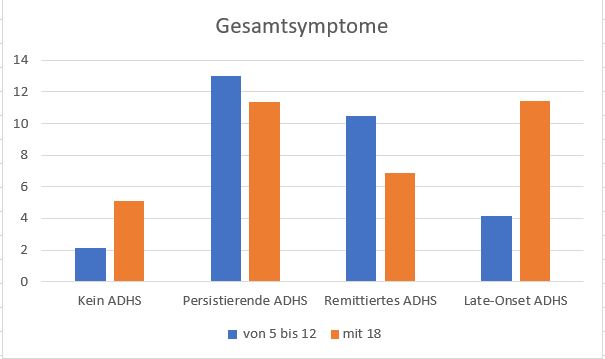
The data from Agnew-Blaits et al., based on a twin cohort study17, provide insight into the development of ADHD symptoms in
- Those not affected
- People with childhood ADHD and ADHD that later goes into remission
- People with persistent childhood ADHD
- (subthreshold) late-onset ADHD
The symptoms reported by each group at ages 5 through 12 are compared with those reported at age 18 (N = 2,040):
 Another study examined the Pelotas Birth Cohort, consisting of N = 5,249 individuals born in Pelotas, Brazil, in 1993, through the ages of 18 to 19; 81.3% of the cohort participated in the study.48
Another study examined the Pelotas Birth Cohort, consisting of N = 5,249 individuals born in Pelotas, Brazil, in 1993, through the ages of 18 to 19; 81.3% of the cohort participated in the study.48
At age 11, 393 children (8.9%) were diagnosed with ADHD. Most of the people with ADHD were male (63.9%).
Among those aged 18 to 19, 492 (12.2%) met all DSM-5 criteria (excluding age at onset). After excluding comorbidities, the prevalence remained at 6.3% (256). It is unclear to us whether women were in the majority here (as stated in the text) or in the minority (as indicated by the figure of 39%).
Both groups exhibited higher rates of traffic accidents, criminal behavior, incarceration, suicide attempts, and comorbidities in adulthood.
However, only 60 children (17.2%) with ADHD still had ADHD at ages 18 to 19, and only 60 young adults (12.6%) with ADHD had already had ADHD at age 11.
The results suggest a discontinuity in ADHD and the possibility of late-onset ADHD. As many as 77.4% of 18- to 19-year-old people with ADHD did not yet have a full-blown case of ADHD at age 11 or earlier.
Several long-term studies spanning 20 to 40 years show that ADHD in children and ADHD in adults often affect distinct groups of people. Among adults, the gender distribution was balanced, whereas among children, there was still a predominance of males. This, too, could suggest a distinction between the two groups.5960616263
The updated 2018 European Consensus on the Diagnosis and Treatment of ADHD in Adults64 notes that many people with ADHDPeople with ADHD have poor memory and therefore find it difficult to recall events and details from their childhood, and that there are reports of adults who document the first onset of symptoms only after the age of 12.6566
A study reports that ADHD that develops later in life tends to be milder.53 This contrasts with reports indicating that women diagnosed late in life, in particular, tend to experience more severe symptoms with significant comorbidities (depression, anxiety).62
The risk of being diagnosed with ADHD for the first time in adulthood also appears to be linked to comorbidities. Comorbidities typical of ADHD that are present in childhood appear to increase the risk of developing ADHD later in life—just as (as has long been known) ADHD in childhood, conversely, increases the risk of developing typical comorbidities in adulthood.6768
A long-term study found that, of 318 children with birth complications, by the age of 40, only 21% of those who had developed ADHD as children still had ADHD; however, they had a lower level of education, more ADHD symptoms, and executive function problems. Among those who had attention problems as children but did not meet the full criteria for ADHD, 6.6% had ADHD by age 40; among those who showed no attention problems as children, 6% had ADHD. Controls without birth complications had a 1.6% prevalence of ADHD at age 40.69 According to these findings, approximately 6 to 6.6% of children with birth complications and 1.6% of those without birth complications could receive an ADHD diagnosis for the first time by age 40.
2.2. Late-onset ADHD: De Novo Late-Onset ADHD
Whether there is a form of ADHD in which no ADHD symptoms were observable during childhood is a matter of debate.
Barkley argues—and we believe he is correct—that symptoms do not necessarily have to have appeared during childhood or adolescence, but can also appear for the first time even after the brain has finished developing (around age 23).
Findings based on the Dunedin Cohort Study—which has been ongoing for more than four decades—go even further. The study found a prevalence of ADHD of 6% in childhood and 3% in adults. However, it also found that the groups with childhood ADHD and adult ADHD barely overlapped, and that many people with adult ADHD had shown no signs of ADHD whatsoever during childhood and adolescence.46 The authors interpret the results as evidence of the existence of two syndromes with different developmental trajectories.
Given that ADHD is a syndrome that can arise from hundreds or even thousands of different causes, we believe that the varying developmental trajectories may also represent different environmental influences. Possible contributors could include certain environmental toxins or diseases that played a role at different times. To investigate this, a study involving multiple birth cohorts from different countries could be helpful.
Among children from families affected by ADHD or ASD, 50% showed no symptoms between the ages of 6 and 12.70 If the age by which the first symptoms must have appeared is set at 16, 99% of people with ADHD are identified, according to a study.7172
According to this, however, one in every hundred cases of ADHD would still have symptoms that first appeared after the age of 16. Assuming a prevalence of ADHD of 8%, this would amount to 64,000 people in Germany; at 5%, there would be 40,000 people with de novo late-onset ADHD that began after age 16.
In most cases, it appears that at least one symptom was highly pronounced during adolescence.73
Furthermore, it cannot be denied that there are environmental factors that can trigger or exacerbate ADHD symptoms even in adulthood. For more on this, see Physical ADHD Risk Factors and Psychological ADHD Risk Factors in the chapter “ : Causes”.
This would be consistent with the hypothesis that the heritability of adult ADHD is lower than that of childhood ADHD. This would suggest that environmental factors may play a greater role in the development of ADHD in adults than in children.874 However, this is contradicted by the fact that the heritability of ADHD in adults was lower only in self-report studies, and that self-report was generally associated with a lower estimate of genetic causes.7576 77 78 79 Differences in the heritability of ADHD depending on the assessment method were also observed between parent ratings (82%), teacher ratings (60%), and self-reports (48%) among 12-year-old twins.78
Regardless, it does not benefit people with ADHD if they are denied treatment in adulthood simply because certain ADHD symptoms were not identified during their childhood. There are no reports indicating that standard treatment methods (particularly stimulants) are less effective or less frequently effective in cases of late-onset ADHD. In this regard, close monitoring by the treating physician may be advisable; however, denying treatment would constitute a violation of the physician’s duty of care. We see this particularly when treatment in adulthood is denied solely because of the lack of elementary school records, even though the symptoms indicate a full-blown case of ADHD.
A study examined 239 participants in the MTA study who had not been diagnosed with ADHD as children and of whom 97 exhibited ADHD symptoms as young adults:80
32 also exhibited the subjective distress required for a diagnosis.
Of these 32, 12 had been diagnosed with ADHD by one of the diagnostic sources available at the time, but not by all of them; as a result of this discrepancy, no diagnosis was made.
Of the remaining 21, the current symptoms in 3 were the result of substance abuse.
Of the remaining 18, 9 already had additional diagnoses of other disorders. In 5 cases, the symptoms were primarily attributed to the other disorder.
Of the 13 cases in which increased ADHD symptoms and impairments first appeared during adolescence, 7 were excluded because their symptoms were reported only by a teacher or by a teacher and the individual themselves.
The study thus identified 6 cases (2.5% of the comparison group without ADHD at the start of the study) of de novo late-onset ADHD in adolescence.
In our view, the study underestimates the prevalence of late-onset ADHD, since it excluded both those for whom even a single source reported ADHD symptoms during childhood and those for whom only a single source reported symptoms during adolescence. Due to this double exclusion, the actual prevalence of late-onset ADHD is likely to be higher.
However, the study conclusively establishes that, even when viewed from the most critical perspective, there is a group of people with late-onset ADHD in late adolescence.81
De novo late-onset ADHD in adolescents is associated with the chronobiological rhythm, which is often delayed in adolescents.82 For more information on the circadian rhythm, see Circadian Rhythms and the Influence of Genes in the article Sleep Problems in ADHD—Neurophysiological Correlates In the section “Neurophysiological Correlates of ADHD” in the chapter Neurological.
2.3. Very Late-Onset ADHD / Senile-Onset / ADHD in Older Adults
A study of 488 consecutive patients admitted to a specialized dementia clinic found ADHD in 7 patients who were initially suspected of having early-onset Alzheimer’s dementia. These 7 people with “very late-onset ADHD” or “senile-onset ADHD” shared four characteristics:83
- significantly younger (< 65 years) than the overall study population
- symptoms primarily related to inattention
- latent manifestation
- a stressful life event prior to the onset of symptoms (stressful experience)
2.4. Late-Onset ADHD in Women
It is relatively common for women to be diagnosed with ADHD only in adulthood. While many more boys than girls are diagnosed during childhood, the ratio is (nearly) equal in adulthood.63
Women who are diagnosed later in life, in particular, experience the most severe symptoms and often suffer from comorbid conditions such as anxiety disorders or depression, which are typical consequences of ADHD that has gone untreated for a long time.
On the other hand, women are more prone to developing emotional disorders that emerge later in life (on average during adolescence), such as depression, dysthymia, various anxiety disorders, or eating disorders. Sex hormones are often cited as possible causes.84
High estrogen levels mitigate deficits in learning and memory.85 This could possibly explain why ADHD symptoms are often not yet detectable in girls during their school years and only become more apparent in women starting at age 35.
One possible mechanism that could explain late-onset symptoms, particularly in women, is the masking effect of estradiol, which declines with age—and especially during menopause—and may then reveal executive function problems. Early-life stress can have lasting effects on the serotonergic circuits that underlie executive function and are unmasked by the loss of estradiol during menopause.86
3. Changes in ADHD Symptoms in Adults
The DSM-IV criteria for ADHD describe the symptoms in children and do not specifically address those in adults.87
The symptoms of ADHD in adults differ significantly from those in children.8889 In particular, hyperactivity decreases significantly. Symptoms such as inner restlessness, an inability to relax, and the “need to be constantly active” come to the fore.
A study reports a linear decline in hyperactivity from 6 to 2.9 points between the ages of 8 and 16.90 Inattention, however, decreased only slightly from 5.8 to 4.9 points over the same period. Nevertheless, the study also discusses a shift in inattention toward executive dysfunction as children age.23
Hyperactivity—measured here using infrared motion sensors while participants were performing attention tests—was still a better discriminator between affected and unaffected adults than attention problems. Even among people with the predominantly inattentive ADHD-I subtype, significantly increased hyperactivity and motor restlessness were observed compared to people without ADHD.91
Adults have far greater opportunities to structure their lives in such a way that the characteristics of ADHD (short attention span, high distractibility, preference for rapid task switching) are no longer a burden but rather an advantage. Children, however—especially at school—must submit to strict external control. The characteristic of people with ADHD (and particularly those with ADHD-HI)—increased intrinsic motivation and reduced extrinsic motivation—is a hindrance in the purely extrinsically motivating school environment.92
For the sake of completeness, it should be noted regarding Friedman that the frustration experienced by people with ADHD when doing something that doesn’t really interest them—and which, as a result, they naturally aren’t particularly good at (which applies to everyone, but to a much greater extent to people with ADHD)—causes significant stress. It is well known that people with ADHD react more intensely to stress. All ADHD symptoms are classic stress symptoms. People with ADHD have an overreactive stress response system.
⇒ ADHD as a Chronic Stress Regulation Disorder
Barkley has compiled a list of typical symptoms of ADHD in adults and verified them through research. Physical hyperactivity decreases significantly, while inner restlessness becomes more apparent. Inattention also decreases significantly.
The following symptoms are most common in adults:
- Inattention (reduced by up to 40% in children)
Attention problems decrease by up to 40% in adults compared to children and adolescents (this decrease is thus smaller than that of the other main symptoms).93 The figures are taken from the data in Biedermann’s publication. We cannot understand why the professional literature interprets this differently. However, the decline in attention problems among adults evident in the data is consistent with our observations (at least among many people with ADHD). One study reports a linear decline in inattention from 5.8 to 4.9 points between the ages of 8 and 16.90
Other sources, however, report an increase in inattention with age9495 , as well as consistent attention problems and executive function problems related to working memory among people aged 60 to 94, some of which were attributed to depression.96 - Hyperactivity (reduced by up to 60% compared to children)
Hyperactivity transforms into inner restlessness in adulthood (Barkley) and decreases by up to 60% compared to children and adolescents9390 We suspect that this is not so much a transformation as it is that, once the hyperactivity subsides, the symptoms of inner tension become more clearly visible. - Impulsivity (reduced by up to 60% when interacting with children)
According to various sources, impulsivity is expected to decrease by up to 60% compared to children and adolescents939790
Another study found no change in impulsivity with age.94 - Emotional overreactivity (more pronounced in adults)98
- Emotional lability99
- Disorganization99
A study identified four patterns regarding hyperactivity and inattention between childhood and adulthood:100
- Hyperactivity
- was low, stay low
- was high, then decreased
- Inattention
- was low, remained low
- was high and continued to rise
Some changes can also be measured neurophysiologically.
While children with hyperactivity exhibit reduced striatal and prefrontal dopamine decarboxylase activity,101 this finding cannot be replicated in adults with ADHD-HI.102 Furthermore, no increase in HVA levels in cerebrospinal fluid is detectable in adults with ADHD. This also suggests that ADHD persisting into adulthood has a different pathophysiological basis.103 However, the HVA level is merely a global measure of dopamine metabolism, whereas in ADHD, dopamine levels in different brain regions must be distinguished.
Adults apparently have a significantly lower number of dopamine transporters in the striatum than children. For every 10 years of age, there is a 7% decline, with the rate of decline being significantly higher up to about age 40 than thereafter. In 50-year-olds, the number of DATs is only about half that of 10-year-olds.104105
At the same time, the number of dopaminergic neurons decreases with age. The amount of phasically released and basal extracellular dopamine in the striatum remains the same.106
According to a study, the problems and limitations on quality of life experienced by older adults with ADHD are similar to those experienced by younger adults with ADHD. This suggests that there is no long-term improvement as a result of continuing to age throughout adulthood.107
Reif, on the other hand, assumes that inattention decreases only slightly, while emotional dysregulation becomes more pronounced in adulthood.108
We believe that emotional dysregulation is generally accepted as a normal trait in children (“immaturity”), whereas it is perceived as inappropriate in adults. We therefore wonder whether emotional dysregulation actually increases in adults with ADHD, or whether children with ADHD may already exhibit emotional instability that is still considered acceptable and therefore not recognized as a symptom of ADHD —just as we suspect is the case with internal tension, which becomes apparent in adulthood after physical hyperactivity subsides. We intend to investigate this in greater depth.
4. Treatment for Adults
In adults, significantly smaller amounts of stimulants are typically required to correct the dopamine and norepinephrine deficit in the reward system and the dlPFC, which may be related to the fact that the excess of dopamine transporters compared to children appears to regress to some extent.
Prescribing an (initial) dose of stimulants equivalent to that used for children would therefore constitute medical malpractice. Regardless of this, treatment with stimulants should always be initiated gradually, starting with the lowest possible doses.
5. ADHD in Older Adults / Seniors
There are only a few studies on the symptoms, diagnosis, and treatment of ADHD in older adults.109110111
Treatment with stimulants is also permitted into old age.112
ADHD medications significantly improve attention even in people with ADHD over 50.113
All clinical trials for stimulants cover only the age range up to 65 years. However, the absence of studies beyond a certain age limit does not automatically constitute off-label use.
Lisdexamfetamine may be routinely prescribed to patients 65 years of age and older. Amphetamine clearance is slightly reduced in older adults. Therefore, a lower dosage should be anticipated.
For MPH, prescribing the drug to patients aged 65 and older constitutes off-label use, but is permitted.
Consequently, the relevant professional associations are not aware of any recourse proceedings initiated by health insurance funds regarding prescriptions issued after the age of 65.
A blanket refusal to prescribe stimulants after a certain age (particularly for those under 65) without a specific, individual reason is likely to constitute a case of medical malpractice.
Edel, Vollmoeller (2006): Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung bei Erwachsenen, Springer Seite 51 ↥
Cortese S, Bellgrove MA, Brikell I, Franke B, Goodman DW, Hartman CA, Larsson H, Levin FR, Ostinelli EG, Parlatini V, Ramos-Quiroga JA, Sibley MH, Tomlinson A, Wilens TE, Wong ICK, Hovén N, Didier J, Correll CU, Rohde LA, Faraone SV (2025): Attention-deficit/hyperactivity disorder (ADHD) in adults: evidence base, uncertainties and controversies. World Psychiatry. 2025 Oct;24(3):347-371. doi: 10.1002/wps.21374. PMID: 40948064; PMCID: PMC12434367. ↥ ↥
Kooij JJ, Michielsen M, Kruithof H, Bijlenga D (2016): ADHD in old age: a review of the literature and proposal for assessment and treatment. Expert Rev Neurother. 2016 Dec;16(12):1371-1381. doi: 10.1080/14737175.2016.1204914. PMID: 27334252. REVIEW ↥
Schlack, Holling, Kurth, Huss (2007): Die Prävalenz der Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung (ADHS) bei Kindern und Jugendlichen in Deutschland. Erste Ergebnisse aus dem Kinder- und Jugendgesundheitssurvey (KiGGS). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007; 50:827-835. ↥
Kessler, Adler, Barkley, Biederman, Conners, Demler, Faraone, Greenhill, Howes, Secnik, Spencer, Ustun, Walters, Zaslavsky (2006): The Prevalence and Correlates of Adult ADHD in the United States: Results From the National Comorbidity Survey Replication; THE AMERICAN JOURNAL OF PSYCHIATRY April 2006 Volume 163, Issue 4, April, 2006, pp. 716-723 ↥
Krause, Krause (2014): ADHS im Erwachsenenalter, Schattauer, Kapitel Prävalenz, S. 9 ff ↥
Fayyad, Sampson, Hwang, Adamowski, Aguilar-Gaxiola, Al-Hamzawi, Andrade, Borges, de Girolamo, Florescu, Gureje, Haro, Hu, Karam, Lee, Navarro-Mateu, O’Neill, Pennell, Piazza, Posada-Villa, Ten Have, Torres, Xavier, Zaslavsky, Kessler; WHO World Mental Health Survey Collaborators (2017): The descriptive epidemiology of DSM-IV Adult ADHD in the World Health Organization World Mental Health Surveys. Atten Defic Hyperact Disord. 2017 Mar;9(1):47-65. doi: 10.1007/s12402-016-0208-3. ↥
Tistarelli, Fagnani, Troianiello, Stazi, Adriani (2019): The nature and nurture of ADHD and its comorbidities: a narrative review on twin studies. Neurosci Biobehav Rev. 2019 Dec 12. pii: S0149-7634(19)30552-4. doi: 10.1016/j.neubiorev.2019.12.017. ↥ ↥
Faraone SV, Biederman J (2005): What is the prevalence of adult ADHD? Results of a population screen of 966 adults. J Atten Disord. 2005 Nov;9(2):384-91. doi: 10.1177/1087054705281478. PMID: 16371661. n = 995 ↥ ↥ ↥ ↥
Kooij JJS, Bijlenga D, Salerno L, Jaeschke R, Bitter I, Balázs J, Thome J, Dom G, Kasper S, Nunes Filipe C, Stes S, Mohr P, Leppämäki S, Casas M, Bobes J, Mccarthy JM, Richarte V, Kjems Philipsen A, Pehlivanidis A, Niemela A, Styr B, Semerci B, Bolea-Alamanac B, Edvinsson D, Baeyens D, Wynchank D, Sobanski E, Philipsen A, McNicholas F, Caci H, Mihailescu I, Manor I, Dobrescu I, Saito T, Krause J, Fayyad J, Ramos-Quiroga JA, Foeken K, Rad F, Adamou M, Ohlmeier M, Fitzgerald M, Gill M, Lensing M, Motavalli Mukaddes N, Brudkiewicz P, Gustafsson P, Tani P, Oswald P, Carpentier PJ, De Rossi P, Delorme R, Markovska Simoska S, Pallanti S, Young S, Bejerot S, Lehtonen T, Kustow J, Müller-Sedgwick U, Hirvikoski T, Pironti V, Ginsberg Y, Félegyházy Z, Garcia-Portilla MP, Asherson P (2019): Updated European Consensus Statement on diagnosis and treatment of adult ADHD. Eur Psychiatry. 2019 Feb;56:14-34. doi: 10.1016/j.eurpsy.2018.11.001. PMID: 30453134. REVIEW ↥
Rajagopal, Duan, Vilar-Ribó, Grove, Zayats, Ramos-Quiroga, Satterstrom, Artigas, Bybjerg-Grauholm, Bækvad-Hansen, Als, Rosengren, Daly, Neale, Nordentoft, Werge, Mors, Hougaard, Mortensen, Ribasés, Børglum, Demontis (2022): Differences in the genetic architecture of common and rare variants in childhood, persistent and late-diagnosed attention-deficit hyperactivity disorder. Nat Genet. 2022 Aug;54(8):1117-1124. doi: 10.1038/s41588-022-01143-7. PMID: 35927488. n = 77.914 ↥ ↥ ↥ ↥
Roselló, Berenguer, Baixauli, Mira, Martinez-Raga, Miranda (2020): Empirical examination of executive functioning, ADHD associated behaviors, and functional impairments in adults with persistent ADHD, remittent ADHD, and without ADHD. BMC Psychiatry. 2020 Mar 24;20(1):134. doi: 10.1186/s12888-020-02542-y. PMID: 32204708; PMCID: PMC7092442. N = 105 ↥ ↥ ↥
Faraone, Biederman, Mick (2006): The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med. 2006 Feb;36(2):159-65. ↥ ↥ ↥
Van Meter AR, Sibley MH, Vandana P, Birmaher B, Fristad MA, Horwitz S, Youngstrom EA, Findling RL, Arnold LE. The stability and persistence of symptoms in childhood-onset ADHD. Eur Child Adolesc Psychiatry. 2023 Jun 4. doi: 10.1007/s00787-023-02235-3. PMID: 37270740. n = 431 ↥ ↥ ↥ ↥
Sibley, Arnold, Swanson, Hechtman, Kennedy, Owens, Molina, Jensen, Hinshaw, Roy, Chronis-Tuscano, Newcorn, Rohde; MTA Cooperative Group (2022): Variable Patterns of Remission From ADHD in the Multimodal Treatment Study of ADHD. Am J Psychiatry. 2022 Feb;179(2):142-151. doi: 10.1176/appi.ajp.2021.21010032. PMID: 34384227; PMCID: PMC8810708. ↥ ↥ ↥
Biederman, Petty, Evans, Small, Faraone (2010): How persistent is ADHD? A controlled 10-year follow-up study of boys with ADHD. Psychiatry Res. 2010 May 30;177(3):299-304. doi: 10.1016/j.psychres.2009.12.010. PMID: 20452063; PMCID: PMC2881837. ↥ ↥
Agnew-Blais, Polanczyk, Danese, Wertz, Moffitt, Arseneault (2016): Evaluation of the Persistence, Remission, and Emergence of Attention-Deficit/Hyperactivity Disorder in Young Adulthood. JAMA Psychiatry. 2016 Jul 1;73(7):713-20. doi: 10.1001/jamapsychiatry.2016.0465. ↥ ↥ ↥
Caye A, Rocha TB, Anselmi L, Murray J, Menezes AM, Barros FC, Gonçalves H, Wehrmeister F, Jensen CM, Steinhausen HC, Swanson JM, Kieling C, Rohde LA (2016): Attention-Deficit/Hyperactivity Disorder Trajectories From Childhood to Young Adulthood: Evidence From a Birth Cohort Supporting a Late-Onset Syndrome. JAMA Psychiatry. 2016 Jul 1;73(7):705-12. doi: 10.1001/jamapsychiatry.2016.0383. PMID: 27192050. n = 5.249 ↥
Mannuzza S, Klein RG, Bessler A, Malloy P, LaPadula M (1998): Adult psychiatric status of hyperactive boys grown up. Am J Psychiatry. 1998 Apr;155(4):493-8. doi: 10.1176/ajp.155.4.493. PMID: 9545994. ↥ ↥
Sibley, Arnold, Swanson, Hechtman, Kennedy, Owens, Molina, Jensen, Hinshaw, Roy, Chronis-Tuscano, Newcorn, Rohde (2021): MTA Cooperative Group. Variable Patterns of Remission From ADHD in the Multimodal Treatment Study of ADHD. Am J Psychiatry. 2021 Aug 13:appiajp202121010032. doi: 10.1176/appi.ajp.2021.21010032. PMID: 34384227. n = 558 ↥ ↥
Grevet EH, Bandeira CE, Vitola ES, de Araujo Tavares ME, Breda V, Zeni G, Teche SP, Picon FA, Salgado CAI, Karam RG, da Silva BS, Sibley MH, Rohde LA, Cupertino RB, Rovaris DL, Bau CHD (2022): The course of attention-deficit/hyperactivity disorder through midlife. Eur Arch Psychiatry Clin Neurosci. 2022 Dec 9. doi: 10.1007/s00406-022-01531-4. PMID: 36484846. ↥ ↥
Barkley, Vortrag (2007): Adult Outcomes of Children with ADHD: The Milwaukee Study. Folien 12/20 und 19/20. ↥
Zeng XW, Hu LF, Cao XL, Yang BR, Wu ZM (2025): Fluctuating course of attention-deficit/hyperactivity disorder across development: Multifactorial influences. World J Psychiatry. 2025 Aug 19;15(8):107780. doi: 10.5498/wjp.v15.i8.107780. PMID: 40837790; PMCID: PMC12362609. REVIEW ↥ ↥ ↥ ↥ ↥
Karam RG, Rovaris DL, Breda V, Picon FA, Victor MM, Salgado CAI, Vitola ES, Mota NR, Silva KL, Meller M, Rohde LA, Grevet EH, Bau CHD (2017): Trajectories of attention-deficit/hyperactivity disorder dimensions in adults. Acta Psychiatr Scand. 2017 Aug;136(2):210-219. doi: 10.1111/acps.12757. PMID: 28555716. ↥
Qiu X, Zhu D, Fu X, Huo Y, Chen X, Zhang J, Wang S, Aisikeer A, Hong X, Lu H, Tang W, Chen J (2025): Longitudinal patterns of attention-deficit/hyperactivity disorder children in Shanghai, China. Sci Rep. 2025 Jun 26;15(1):20305. doi: 10.1038/s41598-025-02254-x. PMID: 40571692; PMCID: PMC12202803. ↥
Miller M, Orme M, Piergies A, Iosif AM, Ozonoff S (2025): Brief Report: Stability of ADHD Symptoms in Early Childhood. J Clin Child Adolesc Psychol. 2025 Jul 23:1-10. doi: 10.1080/15374416.2025.2534939. PMID: 40700722; PMCID: PMC12345110. N = 66 ↥
Pingault JB, Viding E, Galéra C, Greven CU, Zheng Y, Plomin R, Rijsdijk F (2015): Genetic and Environmental Influences on the Developmental Course of Attention-Deficit/Hyperactivity Disorder Symptoms From Childhood to Adolescence. JAMA Psychiatry. 2015 Jul;72(7):651-8. doi: 10.1001/jamapsychiatry.2015.0469. PMID: 25945901; PMCID: PMC6328013. ↥
Greven CU, Asherson P, Rijsdijk FV, Plomin R (2011): A longitudinal twin study on the association between inattentive and hyperactive-impulsive ADHD symptoms. J Abnorm Child Psychol. 2011 Jul;39(5):623-32. doi: 10.1007/s10802-011-9513-7. PMID: 21494861. ↥
Chang Z, Lichtenstein P, Asherson PJ, Larsson H (2013): Developmental twin study of attention problems: high heritabilities throughout development. JAMA Psychiatry. 2013 Mar;70(3):311-8. doi: 10.1001/jamapsychiatry.2013.287. PMID: 23303526. ↥
Rovira P, Demontis D, Sánchez-Mora C, Zayats T, Klein M, Mota NR, Weber H, Garcia-Martínez I, Pagerols M, Vilar-Ribó L, Arribas L, Richarte V, Corrales M, Fadeuilhe C, Bosch R, Martin GE, Almos P, Doyle AE, Grevet EH, Grimm O, Halmøy A, Hoogman M, Hutz M, Jacob CP, Kittel-Schneider S, Knappskog PM, Lundervold AJ, Rivero O, Rovaris DL, Salatino-Oliveira A, da Silva BS, Svirin E, Sprooten E, Strekalova T; ADHD Working Group of the Psychiatric Genomics Consortium; 23andMe Research team; Arias-Vasquez A, Sonuga-Barke EJS, Asherson P, Bau CHD, Buitelaar JK, Cormand B, Faraone SV, Haavik J, Johansson SE, Kuntsi J, Larsson H, Lesch KP, Reif A, Rohde LA, Casas M, Børglum AD, Franke B, Ramos-Quiroga JA, Soler Artigas M, Ribasés M (2020): Shared genetic background between children and adults with attention deficit/hyperactivity disorder. Neuropsychopharmacology. 2020 Sep;45(10):1617-1626. doi: 10.1038/s41386-020-0664-5. PMID: 32279069; PMCID: PMC7419307. METASTUDY ↥
Deng WQ, Elsayed M, Belisario KL, Sanchez-Roige S, Palmer AA, MacKillop J (2025): Genome-Wide Association Studies of Delay Discounting and Impulsive Personality Traits in Children From the Adolescent Behavior and Cognitive Development Study. Genes Brain Behav. 2025 Aug;24(4):e70033. doi: 10.1111/gbb.70033. PMID: 40847891; PMCID: PMC12374252. ↥
Barkley, Murphy, Fischer (2008). ADHD in Adults: What the Science Says. New York: Guilford, Seite 436 ↥ ↥ ↥ ↥ ↥ ↥
Kim, King, Jennings (2019): ADHD remission, inclusive special education, and socioeconomic disparities. SSM Popul Health. 2019 May 30;8:100420. doi: 10.1016/j.ssmph.2019.100420. eCollection 2019 Aug. ↥
Hartman, Rommelse, van der Klugt, Wanders, Timmerman (2019): Stress Exposure and the Course of ADHD from Childhood to Young Adulthood: Comorbid Severe Emotion Dysregulation or Mood and Anxiety Problems. J Clin Med. 2019 Nov 1;8(11). pii: E1824. doi: 10.3390/jcm8111824. n = 609 ↥
Björkenstam, Björkenstam, Jablonska, Kosidou (2018): Cumulative exposure to childhood adversity, and treated attention deficit/hyperactivity disorder: a cohort study of 543 650 adolescents and young adults in Sweden. Psychol Med. 2018 Feb;48(3):498-507. doi: 10.1017/S0033291717001933. ↥
Sibley, Ortiz, Graziano, Dick, Estrada (2019): Metacognitive and motivation deficits, exposure to trauma, and high parental demands characterize adolescents with late-onset ADHD. Eur Child Adolesc Psychiatry. 2019 Aug 6. doi: 10.1007/s00787-019-01382-w. ↥
Braus (2004) EinBlick ins Gehirn ä eine andere Einführung in die Psychiatrie. S. 19 ↥
Braus (2004) EinBlick ins Gehirn – eine andere Einführung in die Psychiatrie. S. 19 ↥
Doering, Lichtenstein, Gillberg, Middeldorp, Bartels, Kuja-Halkola, Lundström (2019): Anxiety at age 15 predicts psychiatric diagnoses and suicidal ideation in late adolescence and young adulthood: results from two longitudinal studies. BMC Psychiatry. 2019 Nov 14;19(1):363. doi: 10.1186/s12888-019-2349-3. n = 14.106 + 9.211 ↥
Sudre, Mangalmurti, Shaw (2018): Growing out of attention deficit hyperactivity disorder: insights from the ‘remitted’ brain. Neurosci Biobehav Rev. 2018 Sep 5. pii: S0149-7634(18)30313-0. doi: 10.1016/j.neubiorev.2018.08.010. ↥ ↥
Sudre, Szekely, Sharp, Kasparek, Shaw (2017): Multimodal mapping of the brain’s functional connectivity and the adult outcome of attention deficit hyperactivity disorder; PNAS October 31, 2017 114 (44) 11787-11792; https://doi.org/10.1073/pnas.1705229114 ↥
Kooij, Bijlenga, Salerno, Jaeschke, Bitter, Balázs, Thome, Dom, Kasper, Filipe, Stes, Mohr, Leppämäki, Brugué, Bobes, Mccarthy, Richarte, Philipsen, Pehlivanidis, Niemela, Styr, Semerci, Bolea-Alamanac, Edvinsson, Baeyens, Wynchank, Sobanski, Philipsen, McNicholas, Caci, Mihailescu, Manor, Dobrescu, Krause, Fayyad, Ramos-Quiroga, Foeken, Rad, Adamou, Ohlmeier, Fitzgerald, Gill, Lensing, Mukaddes, Brudkiewicz, Gustafsson, Tania, Oswald, Carpentier, De Rossi, Delorme, Simoska, Pallanti, Young, Bejerot, Lehtonen, Kustow, Müller-Sedgwick, Hirvikoski, Pironti, Ginsberg, Félegeházy, Garcia-Portilla, Asherson (2018): Updated European Consensus Statement on diagnosis and treatment of adult ADHD, European Psychiatrie, European Psychiatry 56 (2019) 14–34, http://dx.doi.org/10.1016/j.eurpsy.2018.11.001 ↥
Schulz, Newcorn, Fan, Tang, Halperin (2005): Brain activation gradients in ventrolateral prefrontal cortex related to persistence of ADHD in adolescent boys. J Am Acad Child Adolesc Psychiatry. 2005 Jan;44(1):47-54. doi: 10.1097/01.chi.0000145551.26813.f9. PMID: 15608543. ↥
Shaw P, Malek M, Watson B, Greenstein D, de Rossi P, Sharp W (2013): Trajectories of cerebral cortical development in childhood and adolescence and adult attention-deficit/hyperactivity disorder. Biol Psychiatry. 2013 Oct 15;74(8):599-606. doi: 10.1016/j.biopsych.2013.04.007. PMID: 23726514; PMCID: PMC5922431. ↥
Liu, Asherson, Viding, Greven, Pingault (2019): Early Predictors of De Novo and Subthreshold Late-Onset ADHD in a Child and Adolescent Cohort. J Atten Disord. 2019 Dec 30:1087054719892888. doi: 10.1177/1087054719892888. ↥ ↥
Moffitt TE, Houts R, Asherson P, Belsky DW, Corcoran DL, Hammerle M, Harrington H, Hogan S, Meier MH, Polanczyk GV, Poulton R, Ramrakha S, Sugden K, Williams B, Rohde LA, Caspi A (2015): Is Adult ADHD a Childhood-Onset Neurodevelopmental Disorder? Evidence From a Four-Decade Longitudinal Cohort Study. Am J Psychiatry. 2015 Oct;172(10):967-77. doi: 10.1176/appi.ajp.2015.14101266. PMID: 25998281; PMCID: PMC4591104. ↥ ↥
Caye, Rocha, Anselmi, Murray, Menezes, Barros, Gonçalves, Wehrmeister, Jensen, Steinhausen, Swanson, Kieling, Rohde (2016): Attention-Deficit/Hyperactivity Disorder Trajectories From Childhood to Young Adulthood: Evidence From a Birth Cohort Supporting a Late-Onset Syndrome. JAMA Psychiatry. 2016 Jul 1;73(7):705-12. doi: 10.1001/jamapsychiatry.2016.0383. ↥ ↥
Caye A, Rocha TB, Anselmi L, Murray J, Menezes AM, Barros FC, Gonçalves H, Wehrmeister F, Jensen CM, Steinhausen HC, Swanson JM, Kieling C, Rohde LA (2016): Attention-Deficit/Hyperactivity Disorder Trajectories From Childhood to Young Adulthood: Evidence From a Birth Cohort Supporting a Late-Onset Syndrome. JAMA Psychiatry. 2016 Jul 1;73(7):705-12. doi: 10.1001/jamapsychiatry.2016.0383. PMID: 27192050. ↥ ↥
Asherson, Agnew-Blais (2019): Annual Research Review: Does late-onset attention-deficit/hyperactivity disorder exist? J Child Psychol Psychiatry. 2019 Mar 7. doi: 10.1111/jcpp.13020. ↥
Müller (2018): Kinder tragen ADHS nur selten ins Erwachsenenalter. Ärztezeitung online 07.06.2018 ↥
Cooper, Hammerton, Collishaw, Langley, Thapar, Dalsgaard, Stergiakouli, Tilling, Davey Smith, Maughan, O’Donovan, Thapar, Riglin (2018): Investigating late-onset ADHD: a population cohort investigation. J Child Psychol Psychiatry. 2018 Oct;59(10):1105-1113. doi: 10.1111/jcpp.12911. ↥
Liu, Li, Viding, Asherson, Pingault (2018): The developmental course of inattention symptoms predicts academic achievement due to shared genetic aetiology: a longitudinal twin study. Eur Child Adolesc Psychiatry. 2019 Mar;28(3):367-375. doi: 10.1007/s00787-018-1200-6. ↥
Murray, Booth, Auyeung, Eisner, Ribeaud, Obsuth (2018): Outcomes of ADHD Symptoms in Late Adolescence: Are Developmental Subtypes Important? J Atten Disord. 2018 Aug 22:1087054718790588. doi: 10.1177/1087054718790588. ↥ ↥
Murray, Eisner, Obsuth, Ribeaud (2017): Identifying Early Markers of “Late Onset” Attention Deficit and Hyperactivity/Impulsivity Symptoms. J Atten Disord. 2017 Apr 1:1087054717705202. doi: 10.1177/1087054717705202. ↥
Pingault, Viding, Galéra, Greven, Zheng, Plomin, Rijsdijk (2015): Genetic and Environmental Influences on the Developmental Course of Attention-Deficit/Hyperactivity Disorder Symptoms From Childhood to Adolescence. JAMA Psychiatry. 2015 Jul;72(7):651-8. doi: 10.1001/jamapsychiatry.2015.0469. n = 8.395 twin pairs ↥
Pingault, Tremblay, Vitaro, Carbonneau, Genolini, Falissard, Côté (2011): Childhood trajectories of inattention and hyperactivity and prediction of educational attainment in early adulthood: a 16-year longitudinal population-based study. Am J Psychiatry. 2011 Nov;168(11):1164-70. doi: 10.1176/appi.ajp.2011.10121732. n = 2.000 ↥
Jurek L, Montègue S, Larrieu A, Icard C, Rolland B (2023): Compared Profile of Late-Onset Versus Childhood-Onset ADHD: A Case-Control Study Among Treatment-Seeking Adult Patients. J Atten Disord. 2023 Aug 11:10870547231191756. doi: 10.1177/10870547231191756. PMID: 37565344. ↥
Esin IS, Turan B, Akıncı MA, Karabak M, Dursun OB (2020): Do we need to re-think on subthreshold childhood psychiatric cases? A follow-up study. Med Hypotheses. 2020 Jun;139:109697. doi: 10.1016/j.mehy.2020.109697. PMID: 32247189. ↥
Moffitt, Houts, Asherson, Belsky, Corcoran, Hammerle, Harrington, Hogan, Meier, Polanczyk, Poulton, Ramrakha, Sugden, Williams, Rohde, Caspi (2015): Is Adult ADHD a Childhood-Onset Neurodevelopmental Disorder? Evidence From a Four-Decade Longitudinal Cohort Study; American Journal of Psychiatry 2015 172:10, 967-977 ↥
Shaw, Polanczyk (2017): Combining epidemiological and neurobiological perspectives to characterize the lifetime trajectories of ADHD. Eur Child Adolesc Psychiatry (2017) 26: 139. https://doi.org/10.1007/s00787-017-0944-8 ↥
Caye, Rocha, Anselmi, Murray, Menezes, Barros, Gonçalves, Wehrmeister, Jensen, Steinhausen, Swanson, Kieling, Rohde (2016): Attention-Deficit/Hyperactivity Disorder Trajectories From Childhood to Young Adulthood: Evidence From a Birth Cohort Supporting a Late-Onset Syndrome. JAMA Psychiatry. 2016 Jul 1;73(7):705-12. doi: 10.1001/jamapsychiatry.2016.0383. ↥
Riglin, Eyre, Thapar, Stringaris, Leibenluft, Pine, Tilling, Smith, O’Donovan, Thapar (2019): Identifying Novel Types of Irritability Using a Developmental Genetic Approach. Am J Psychiatry. 2019 Aug 1;176(8):635-642. doi: 10.1176/appi.ajp.2019.18101134. ↥ ↥
London, Landes (2019): Cohort Change in the Prevalence of ADHD Among U.S. Adults: Evidence of a Gender-Specific Historical Period Effect. J Atten Disord. 2019 Jun 13:1087054719855689. doi: 10.1177/1087054719855689. ↥ ↥
Kooij, Bijlenga, Salerno, Jaeschke, Bitter, Balázs, Thome, Dom, Kasper, Filipe, Stes, Mohr, Leppämäki, Brugué, Bobes, Mccarthy, Richarte, Philipsen, Pehlivanidis, Niemela, Styr, Semerci, Bolea-Alamanac, Edvinsson, Baeyens, Wynchank, Sobanski, Philipsen, McNicholas, Caci, Mihailescu, Manor, Dobrescu, Krause, Fayyad, Ramos-Quiroga, Foeken, Rad, Adamou, Ohlmeier, Fitzgerald, Gill, Lensing, Mukaddes, Brudkiewicz, Gustafsson, Tania, Oswald, Carpentier, De Rossi, Delorme, Simoska, Pallanti, Young, Bejerot, Lehtonen, Kustow, Müller-Sedgwick, Hirvikoski, Pironti, Ginsberg, Félegeházy, Garcia-Portilla, Asherson (2018): Updated European Consensus Statement on diagnosis and treatment of adult ADHD, European Psychiatrie, European Psychiatry 56 (2019) 14–34, http://dx.doi.org/10.1016/j.eurpsy.2018.11.001, Seite 17 ↥
Faraone, Kunwar, Adamson, Biederman (2009): Personality traits among ADHD adults: implications of late-onset and subthreshold diagnoses; Psychol Med. 2009 Apr; 39(4): 685–693. doi: [10.1017/S0033291708003917]; PMCID: PMC2874959; NIHMSID: NIHMS199982; PMID: 18588742 ↥
Chandra, Biederman, Faraone (2016): Assessing the Validity of the Age at Onset Criterion for Diagnosing ADHD in DSM-5; J Atten Disord. 2016 Feb 27. pii: 1087054716629717. ↥
Plana-Ripoll, Pedersen, Holtz, Benros, Dalsgaard, de Jonge, Fan, Degenhardt, Ganna, Greve, Gunn, Iburg, Kessing, Lee, Lim, Mors, Nordentoft, Prior, Roest, Saha, Schork, Scott, Scott, Stedman, Sørensen, Werge, Whiteford, Laursen, Agerbo, Kessler, Mortensen, McGrath (2019): Exploring Comorbidity Within Mental Disorders Among a Danish National Population. JAMA Psychiatry. 2019;76(3):259-270. doi:10.1001/jamapsychiatry.2018.3658 201976(3):259–270. ↥
Polanczyk, Casella, Jaffee (2019): Commentary: ADHD lifetime trajectories and the relevance of the developmental perspective to Psychiatry: reflections on Asherson and Agnew-Blais. J Child Psychol Psychiatry. 2019 Apr;60(4):353-355. doi: 10.1111/jcpp.13050. ↥
Schiavone, Virta, Leppämäki, Launes, Vanninen, Tuulio-Henriksson, Immonen, Järvinen, Lehto, Michelsson, Hokkanen (2019): ADHD and subthreshold symptoms in childhood and life outcomes at 40 years in a prospective birth-risk cohort. Psychiatry Res. 2019 Sep 25;281:112574. doi: 10.1016/j.psychres.2019.112574. ↥
Charman T, Bazelmans T, Pasco G, Begum Ali J, Johnson MH, Jones EJH; BASIS/STAARS Team (2026): Mid-childhood developmental and behavioural outcomes in infants with a family history of autism and/or attention deficit hyperactivity disorder. J Child Psychol Psychiatry. 2026 Feb;67(2):282-295. doi: 10.1111/jcpp.70048. PMID: 40923413; PMCID: PMC12812788. n = 263 ↥
Kieling, Kieling, Rohde, Frick, Moffitt, Nigg, Tannock, Castellanos (2010): Am J Psychiatry. 2010 Jan;167(1):14-6. doi: 10.1176/appi.ajp.2009.09060796. ↥
Asherson P, Agnew-Blais J (2019): Annual Research Review: Does late-onset attention-deficit/hyperactivity disorder exist? J Child Psychol Psychiatry. 2019 Apr;60(4):333-352. doi: 10.1111/jcpp.13020. PMID: 30843223. REVIEW ↥
Kooij JJS, Bijlenga D, Salerno L, Jaeschke R, Bitter I, Balázs J, Thome J, Dom G, Kasper S, Nunes Filipe C, Stes S, Mohr P, Leppämäki S, Casas M, Bobes J, Mccarthy JM, Richarte V, Kjems Philipsen A, Pehlivanidis A, Niemela A, Styr B, Semerci B, Bolea-Alamanac B, Edvinsson D, Baeyens D, Wynchank D, Sobanski E, Philipsen A, McNicholas F, Caci H, Mihailescu I, Manor I, Dobrescu I, Saito T, Krause J, Fayyad J, Ramos-Quiroga JA, Foeken K, Rad F, Adamou M, Ohlmeier M, Fitzgerald M, Gill M, Lensing M, Motavalli Mukaddes N, Brudkiewicz P, Gustafsson P, Tani P, Oswald P, Carpentier PJ, De Rossi P, Delorme R, Markovska Simoska S, Pallanti S, Young S, Bejerot S, Lehtonen T, Kustow J, Müller-Sedgwick U, Hirvikoski T, Pironti V, Ginsberg Y, Félegyházy Z, Garcia-Portilla MP, Asherson P (2019): Updated European Consensus Statement on diagnosis and treatment of adult ADHD. Eur Psychiatry. 2019 Feb;56:14-34. doi: 10.1016/j.eurpsy.2018.11.001. PMID: 30453134. Page 20 ↥
Larsson H, Asherson P, Chang Z, Ljung T, Friedrichs B, Larsson JO, Lichtenstein P (2013): Genetic and environmental influences on adult attention deficit hyperactivity disorder symptoms: a large Swedish population-based study of twins. Psychol Med. 2013 Jan;43(1):197-207. doi: 10.1017/S0033291712001067. PMID: 22894944. ↥
Brikell I, Kuja-Halkola R, Larsson H (2015): Heritability of attention-deficit hyperactivity disorder in adults. Am J Med Genet B Neuropsychiatr Genet. 2015 Sep;168(6):406-413. doi: 10.1002/ajmg.b.32335. PMID: 26129777. REVIEW ↥
Kan KJ, Dolan CV, Nivard MG, Middeldorp CM, van Beijsterveldt CE, Willemsen G, Boomsma DI (2013): Genetic and environmental stability in attention problems across the lifespan: evidence from the Netherlands twin register. J Am Acad Child Adolesc Psychiatry. 2013 Jan;52(1):12-25. doi: 10.1016/j.jaac.2012.10.009. PMID: 23265630. REVIEW ↥
Du Rietz E, Cheung CH, McLoughlin G, Brandeis D, Banaschewski T, Asherson P, Kuntsi J (2016): Self-report of ADHD shows limited agreement with objective markers of persistence and remittance. J Psychiatr Res. 2016 Nov;82:91-9. doi: 10.1016/j.jpsychires.2016.07.020. PMID: 27478936; PMCID: PMC5036506. ↥
Merwood A, Greven CU, Price TS, Rijsdijk F, Kuntsi J, McLoughlin G, Larsson H, Asherson PJ (2013): Different heritabilities but shared etiological influences for parent, teacher and self-ratings of ADHD symptoms: an adolescent twin study. Psychol Med. 2013 Sep;43(9):1973-84. doi: 10.1017/S0033291712002978. PMID: 23298428; PMCID: PMC3818571. ↥ ↥
Faraone, Larsson (2019): Genetics of attention deficit hyperactivity disorder. Mol Psychiatry. 2019 Apr;24(4):562-575. doi: 10.1038/s41380-018-0070-0. PMID: 29892054; PMCID: PMC6477889. REVIEW ↥
Sibley MH, Rohde LA, Swanson JM, Hechtman LT, Molina BSG, Mitchell JT, Arnold LE, Caye A, Kennedy TM, Roy A, Stehli A; Multimodal Treatment Study of Children with ADHD (MTA) Cooperative Group (2018): Late-Onset ADHD Reconsidered With Comprehensive Repeated Assessments Between Ages 10 and 25. Am J Psychiatry. 2018 Feb 1;175(2):140-149. doi: 10.1176/appi.ajp.2017.17030298. PMID: 29050505; PMCID: PMC5814300. ↥
Ilario C1, Alt A1, Bader M2, Sentissi (2019): Can ADHD have an adulthood onset? (Article in French). Encephale. 2019 Jun 26. pii: S0013-7006(19)30206-4. doi: 10.1016/j.encep.2019.05.004. ↥
Lunsford-Avery JR, Kollins SH (2018): Editorial Perspective: Delayed circadian rhythm phase: a cause of late-onset attention-deficit/hyperactivity disorder among adolescents? J Child Psychol Psychiatry. 2018 Dec;59(12):1248-1251. doi: 10.1111/jcpp.12956. PMID: 30176050; PMCID: PMC6487490. ↥
Sasaki, Jono, Fukuhara, Honda, Ishikawa, Boku, Takebayashi (2022): Late-manifestation of attention-deficit/hyperactivity disorder in older adults: an observational study. BMC Psychiatry. 2022 May 24;22(1):354. doi: 10.1186/s12888-022-03978-0. PMID: 35610630; PMCID: PMC9128193. ↥
Martel MM, Klump K, Nigg JT, Breedlove SM, Sisk CL (2009): Potential hormonal mechanisms of attention-deficit/hyperactivity disorder and major depressive disorder: a new perspective. Horm Behav. 2009 Apr;55(4):465-79. doi: 10.1016/j.yhbeh.2009.02.004. PMID: 19265696; PMCID: PMC3616481. ↥
Iqbal J, Huang GD, Xue YX, Yang M, Jia XJ (2024): Role of estrogen in sex differences in memory, emotion and neuropsychiatric disorders. Mol Biol Rep. 2024 Mar 12;51(1):415. doi: 10.1007/s11033-024-09374-z. PMID: 38472517. REVIEW ↥
Shanmugan S, Loughead J, Cao W, Sammel MD, Satterthwaite TD, Ruparel K, Gur RC, Epperson CN (2017): Impact of Tryptophan Depletion on Executive System Function during Menopause is Moderated by Childhood Adversity. Neuropsychopharmacology. 2017 Nov;42(12):2398-2406. doi: 10.1038/npp.2017.64. PMID: 28322235; PMCID: PMC5645747. ↥
Barkley, der an der Kriterienerstellung des DSM IV mitgewirkt hat, in Barkley, Benton (2012, 2017): Das große Handbuch für Erwachsene mit ADHS ↥
Barkley, Benton (2012, 2017): Das große Handbuch für Erwachsene mit ADHS ↥
Edel, Vollmoeller (2006): Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung bei Erwachsenen, Springer, Seite 46 ↥
Pingault, Viding, Galéra, Greven, Zheng, Plomin, Rijsdijk (2015): Genetic and Environmental Influences on the Developmental Course of Attention-Deficit/Hyperactivity Disorder Symptoms From Childhood to Adolescence. JAMA Psychiatry. 2015 Jul;72(7):651-8. doi: 10.1001/jamapsychiatry.2015.0469. ↥ ↥ ↥ ↥
Teicher, Polcar, Fourligas, Vitaliano, Navalta (2012): Hyperactivity persists in male and female adults with ADHD and remains a highly discriminative feature of the disorder: a case-control study. BMC Psychiatry. 2012 Nov 7;12:190. doi: 10.1186/1471-244X-12-190. PMID: 23134619; PMCID: PMC3560176. N = 100 ↥
so auch Friedmann, in New York Times Online: A Natural Fix on A.D.H.D, Sunday Review, 31.10.2014 ↥
Edel, Vollmoeller (2006): Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung bei Erwachsenen, Springer, Seite 51, mit Verweis auf Biederman, Mick, Faraone (2000): Age-dependent decline of symptoms of attention deficit hyperactivity disorder: impact of remission definition and symptom type. Am J Psychiatry 157:816–818 ↥ ↥ ↥
Bijlenga, Ulberstad, Thorell, Christiansen, Hirsch, Kooij (2019): Objective assessment of attention-deficit/hyperactivity disorder in older adults compared with controls using the QbTest. Int J Geriatr Psychiatry. 2019 Jun 26. doi: 10.1002/gps.5163. ↥ ↥
Ciftci E, Alp ZB (2025): Quantitative EEG Insights Into A Hundred Adult ADHD Patients: A Deep Dive Into Test of Variables of Attention (TOVA) Correlations and Attention Dynamics. CNS Neurosci Ther. 2025 Mar;31(3):e70304. doi: 10.1111/cns.70304. PMID: 40103194; PMCID: PMC11919765. ↥
Semeijn, Korten, Comijs, Michielsen, Deeg, Beekman, Kooij (2015) No lower cognitive functioning in older adults with attention-deficit/hyperactivity disorder. Int Psychogeriatr. 2015 Sep;27(9):1467-76. doi: 10.1017/S1041610215000010. ↥
Areces, García, Cueli, Rodríguez (2019): Is a Virtual Reality Test Able to Predict Current and Retrospective ADHD Symptoms in Adulthood and Adolescence? Brain Sci. 2019 Oct 13;9(10). pii: E274. doi: 10.3390/brainsci9100274. ↥
Edel, Vollmoeller (2006): Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung bei Erwachsenen, Springer, Seite 82, mit Verweis auf Biederman, Mick, Faraone (2000): Age-dependent decline of symptoms of attention deficit hyperactivity disorder: impact of remission definition and symptom type. Am J Psychiatry 157:816–818 ↥
Edel, Vollmoeller (2006): Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung bei Erwachsenen, Springer, Seite 82, mwN ↥ ↥
Larsson H, Dilshad R, Lichtenstein P, Barker ED (2011): Developmental trajectories of DSM-IV symptoms of attention-deficit/hyperactivity disorder: genetic effects, family risk and associated psychopathology. J Child Psychol Psychiatry. 2011 Sep;52(9):954-63. doi: 10.1111/j.1469-7610.2011.02379.x. PMID: 21434915. ↥
Ernst, Zametkin, Matochik, Jons, Cohen (1998): DOPA decarboxylase activity in attention deficit hyperactivity disorder adults. A (fluorine-18) fluorodopa positron emission tomographic study; J. Neurosci. 18, 5901-5907, 1998 zitiert nach Franck (2003): Hyperaktivität und Schizophrenie – eine explorative Studie; Dissertation, Seite 68 ↥
Franck (2003): Hyperaktivität und Schizophrenie – eine explorative Studie; Dissertation, Seite 68 ↥
Ernst, Liebenauer, Tebeka, Jons, Eisenhofer, Murphy, Zametkin (1997): Selegiline in ADHD adults: Plasma monoamine and monoamine metabolites. Neuropsychopharmacology 16, 276-284, 1997, zitiert nach Franck (2003): Hyperaktivität und Schizophrenie – eine explorative Studie; Dissertation, Seite 68 ↥
Krause, Krause (2014): ADHS im Erwachsenenalter, Schattauer, Seite 232, mit etlichen Nachweisen ↥
Dougherty, Bonab, Spencer, Rauch, Madras, Fischman (1999): Dopamine transporter density in patients with attention deficit hyperactivity disorder. Lancet 354: 2132-2133; PDF in The Lancet 354(9196):2132-3; DOI: 10.1016/S0140-6736(99)04030-1 ↥
Speranza L, di Porzio U, Viggiano D, de Donato A, Volpicelli F (2021): Dopamine: The Neuromodulator of Long-Term Synaptic Plasticity, Reward and Movement Control. Cells. 2021 Mar 26;10(4):735. doi: 10.3390/cells10040735. PMID: 33810328; PMCID: PMC8066851. REVIEW ↥
Thorell, Holst, Sjöwall (2019): Quality of life in older adults with ADHD: links to ADHD symptom levels and executive functioning deficits. Nord J Psychiatry. 2019 Aug 5:1-8. doi: 10.1080/08039488.2019.1646804. ↥
Vortrag Andreas Reif (2017): Fokus ADHS, Minute 29 ↥
Dobrosavljevic M, Larsson H, Cortese S (2023): The diagnosis and treatment of attention-deficit hyperactivity disorder (ADHD) in older adults. Expert Rev Neurother. 2023 Jul-Dec;23(10):883-893. doi: 10.1080/14737175.2023.2250913. PMID: 37725058. REVIEW ↥
Goodman DW, Mitchell S, Rhodewalt L, Surman CB (2016): Clinical Presentation, Diagnosis and Treatment of Attention-Deficit Hyperactivity Disorder (ADHD) in Older Adults: A Review of the Evidence and its Implications for Clinical Care. Drugs Aging. 2016 Jan;33(1):27-36. doi: 10.1007/s40266-015-0327-0. PMID: 26659731. REVIEW ↥
Wudy S, Mauche N, Huang J, Strauß M (2025) Behandlung einer Aufmerksamkeitsdefizit-Hyperaktivitätsstörung (ADHS) im höheren Lebensalter – Für ADHS ist es nie zu spät. Nervenarzt 2025 · 96:300–303https://doi.org/10.1007/s00115-025-01807-9 german ↥
Döpfner M, Banascheski T, Rösler M, Skrodzki K: Stellungnahme des zentralen adhs-netzeszur Pharmakologischen Behandlung von Aufmerksamkeitsdefizit- / Hyperaktivitätsstörungen (ADHS) bei Senioren german ↥
Lensing MB, Zeiner P, Sandvik L, Opjordsmoen S (2015): Psychopharmacological treatment of ADHD in adults aged 50+: an empirical study. J Atten Disord. 2015 May;19(5):380-9. doi: 10.1177/1087054714527342. PMID: 24681898. ↥