
Amphetamine-based medications (AMP) for ADHD
Due to the responder/non-responder profile that differs from that of MPH, amphetamine medications are particularly suitable—regardless of age—for people with ADHD who do not respond to MPH, and they are clearly preferable to the use of non-stimulants (e.g., noradrenergic medications or tricyclic antidepressants).1 A summary of several studies reports a 69% response rate to amphetamine-based medications and a 59% response rate to methylphenidate. 87% of people with ADHD responded to one of the two types of active ingredients.2
Amphetamine-based medications are also—(even) more so than MPH—suitable for the adjunctive treatment of comorbid dysphoria or depression. For more on this, see Stimulant monotherapy as a first step in treating comorbid depression and ADHD] In the article Choice of medication for ADHD or ADHD with comorbid conditions.
In December 2025, we replaced the outdated spelling “Amphetamin” with the modern spelling “Amfetamin.”
1. Active Ingredients in Amphetamine-Based Medications
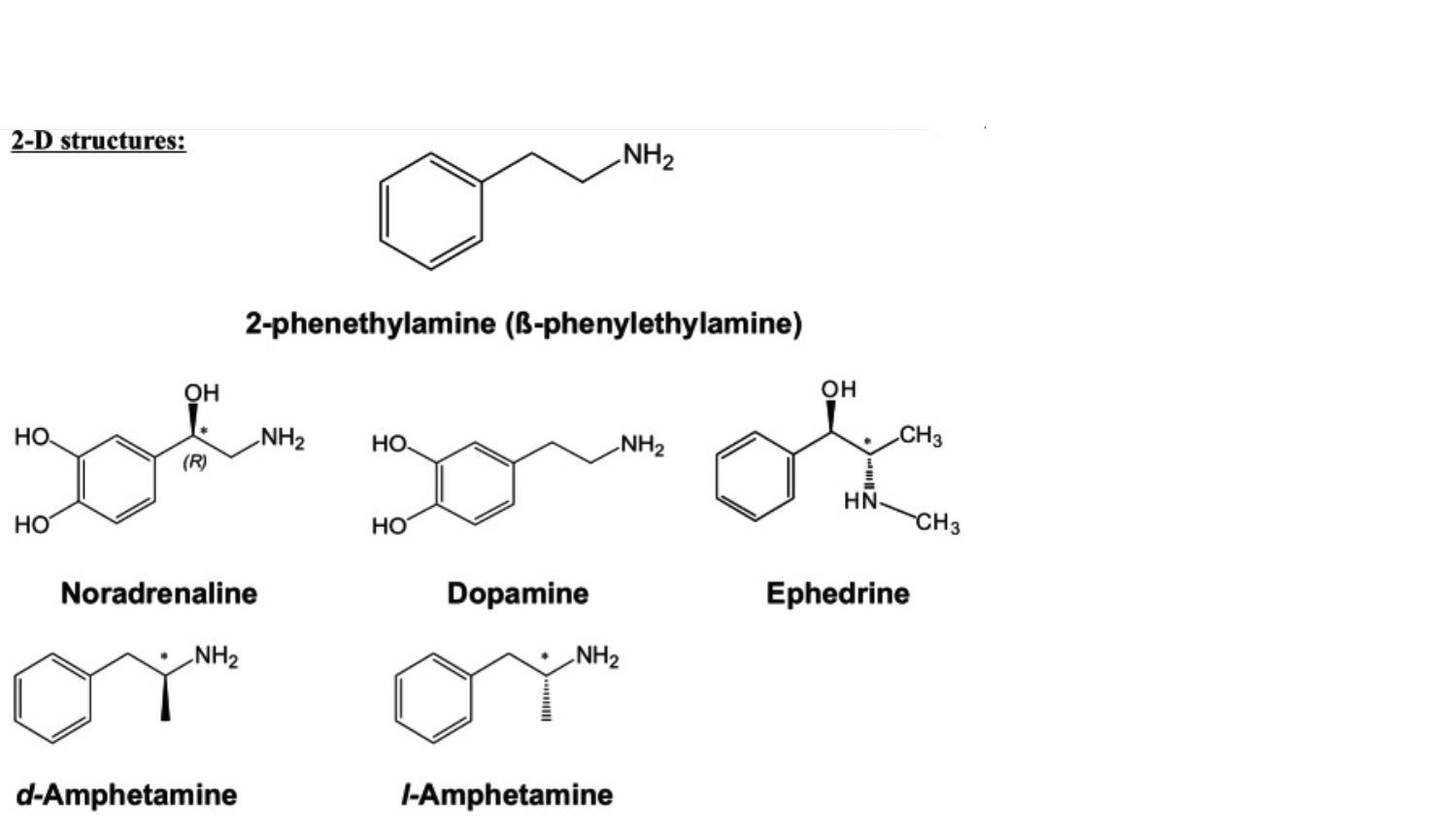
AMP has a chiral center with two enantiomers:3
- Levo-AMP (l-AMP, levorotatory)
- Norepinephrine release as strong as or stronger than d-AMP
- Dextro-AMP (d-AMP, dextrorotatory)
- higher dopamine release than l-AMP
Around 1976, it became known that dextroamphetamine—the purely dextrorotatory isomer, which was marketed at the time as Dexedrine—was more effective in treating ADHD symptoms than the racemic mixture Benzedrine (racemate: a mixture of levorotatory = L-Amp and dextrorotatory = D-Amp amphetamine isomers).4
The d-isomer is four times as effective at releasing dopamine as the l-isomer, while norepinephrine is released equally by both isomers or, in the case of L-amphetamine, even slightly more strongly.4
The amphetamine mixed-salt preparations available in the United States, which consist of equal parts of racemic d,l-AMP sulfate, d,l-AMP aspartate monohydrate, and two enantiomerically pure d-AMP salts (d-AMP sulfate and d-AMP saccharate)—resulting in a 3:1 ratio of d-AMP to l-AMP isomers and salts—exhibit a relatively greater release of norepinephrine than pure d-AMP, although, in absolute terms, dopamine release is still greater than norepinephrine release.
The following factors are relevant to ADHD treatment:
1.1. Dextroamphetamine (D-amphetamine)
Dextroamphetamine (the dextrorotatory isomer) is also called dexamphetamine or S-(+)-amphetamine.
Dextroamphetamine is the dextrorotatory (D-) enantiomer of amphetamine, as opposed to the levorotatory levoamphetamine (see below).
Dextroamphetamine sulfate is the salt form of dextroamphetamine.
D-amphetamine medications have a 3- to 4-fold stronger effect on the central nervous system than racemic amphetamine medications, while also having a weaker sympathomimetic effect in the periphery; for this reason, D-amphetamine medications are preferred for the treatment of ADHD.5
D-amphetamine causes approximately 3 to 4 times the dopamine release compared to L-amphetamine, while the noradrenergic effect is roughly the same or half as strong.67 8 4
This opens up the possibility of formulating the medication with a pronounced dopaminergic effect (dexamfetamine) or with a balanced dopaminergic and noradrenergic effect to a slightly noradrenergic-dominant effect (levamfetamine).
D-amphetamine is more stimulating than MPH and is therefore the preferred treatment for ADHD-I.9
Even in cases of comorbid dysthymia, dysphoria, or depression, it is often more effective than MPH due to its noticeable serotonergic effect10.
1.1.1. Dextroamphetamine without a lysine bond
Brand names: Attentin (Germany, since late 2011), Dexamin (Switzerland: as a compounded prescription), Philla (Austria), Dexedrin
The medication is effective for about 6 hours, so it is usually necessary to take it twice a day.
Increased potential for misuse due to the absence of a lysine bond.Medice (2017): Attentin® – Guide for Prescribing Physicians
Not approved for adults in Germany, so it is used off-label. Reimbursement by health insurance companies is very difficult. Approval for adults has been requested,
The half-life of the D-enantiomer is11
- 9 hours for children ages 6 to 12
- 11 hours for adolescents aged 13 to 17
- 10 hours for adults
Dextroamphetamine binds to transporters with KI (lower = stronger):12
NET: 39–55
DAT: 34 - 225
SERT: 1441 - 3830
1.1.2. Dextroamphetamine derived from lisdexamfetamine (with a lysine moiety)
Lisdexamfetamine (LDX) is a prodrug of D-amphetamine that is bound to L-lysine, forming a substance that is inactive on its own. Lisdexamfetamine is therefore an active ingredient that is only converted into the actually active substance—in this case, D-amphetamine—once inside the body. As a result, the risk of abuse is very low.13 The subjective effects of intravenous administration are identical to those of oral administration, and the Cmax of D-amphetamine is also identical.4 This drastically reduces the risk of abuse. Nevertheless, the effect is linearly dose-dependent up to 250 mg. LDX therefore does not offer protection against overdose.14
In its natural L-form, lysine is an essential proteinogenic α-amino acid. Its enantiomer, D-lysine, does not occur in natural proteins.
In lisdexamfetamine, the amino group of D-amphetamine is linked to the carbonyl group of L-lysine via an amide bond.
Lisdexamfetamine (LDX) bound to lysine is rapidly absorbed into the bloodstream from the small intestine. This occurs via active transport, presumably predominantly via the peptide transporter 1 (PEPT1), although LDX has a higher affinity for PEPT2.12 Enzymatic hydrolysis of the peptide bond to release d-amphetamine into the blood occurs in the lysate and in the cytosolic extract of human erythrocytes, but not in the membrane fraction. This conversion is strongly inhibited by a protease inhibitor cocktail, bestatin, and ethylenediaminetetraacetic acid, suggesting that an aminopeptidase is responsible for the hydrolytic cleavage of the LDX peptide bond. It does not appear to be aminopeptidase B.15
Not every prodrug in which an active ingredient is linked to another chemical moiety via an amide bond is hydrolyzed in vivo at a predictable rate. There are also amphetamine derivatives with amide bonds in which the amide bond is not cleaved in vivo (within a useful timeframe).16
Due to the necessary and slow conversion step from LDX to d-AMP, the effect occurs approximately 1 hour later than when d-AMP sulfate is taken.14 Unlike the hydrophilic LDX, the lipophilic and pharmacologically active d-AMP crosses the blood-brain barrier and enters the CNS, where it exerts its effects.312
Since the effect remains fairly consistent throughout the duration of action, the unpleasant rebound effects commonly associated with MPH (short-term increased restlessness as the effect wears off) do not occur or are significantly milder.
The effect is equivalent to that of D-amphetamine. A conversion table from dexamphetamine to Vyvanse can be found on ADHSpedia.17 Additional conversion tables are available from Kühle18 and, for American formulations, from Stutzman et al.19
Trade names:
- Vyvanse (EU, since late 2013, for children, 20, 30, 40, 50, 60, 70 mg)20
- Vyvanse Adult (EU, since May 1, 2019, for adults, 30, 50, 70 mg)20. Since 2023, 20, 40, and 60 mg doses have also been approved in Germany.
- Vyvanse and Vyvanse Adult were combined in 2023 into a single drug with a unified marketing authorization. The two had already been identical products. Since March 2024, Vyvanse has been available in Germany in 20, 30, 40, 50, 60, and 70 mg doses for children and adults.
- Vyvanse (U.S.) is available in doses ranging from 10 mg to 70 mg21
- Tyvense (U.S.) is available in doses ranging from 20 mg to 70 mg
- Teva Lisdexamfetamine (Canada) is available in doses of 10 mg, 20 mg, 30 mg, 40 mg, 50 mg, 60 mg, and 70 mg22
Generic Drugs:
- Lisdexamfetamine has been available in Germany as a generic drug (e.g., Lisdexamfetamine Ratiopharm) since August 2024, and 100-capsule packages are also on the market.
Lisdexamfetamine has only been classified as a controlled substance in Germany since 2013.
Austria appears to be the only country where, as of 2023, Vyvanse is not classified as a narcotic (Austrian term: Suchtgift).23
Lisdexamfetamine is also approved in the United States for the treatment of binge eating.24
Due to its long-lasting effect, dextroamphetamine reaches a steady state. Steady state appears to be reached on day 5.25 The consequences are that, when administering lisdexamfetamine—as with dextroamphetamine—dose titrations should not be conducted at intervals shorter than one week.
| Lisdexamfetamine dimesylate (capsule, e.g., Vyvanse) | Dextroamphetamine sulfate (tablet, e.g., Attentin) | Dextroamphetamine base (pharmacologically active) | Lisdexamfetamine base (irrelevant) |
|---|---|---|---|
| 10 mg | 2.95 mg | 5.78 mg | |
| 5 mg | 3.67 mg | ||
| 20 mg | 8.04 mg | 5.90 mg | 11.56 mg |
| 10 mg | 7.39 mg | ||
| 30 mg | 12.06 mg | 8.85 mg | 17.34 mg |
| 40 mg | 16.08 mg | 11.80 mg | 23.12 mg |
| 20 mg | 14.68 mg | ||
| 50 mg | 20.10 mg | 14.75 mg | 28.90 mg |
| 60 mg | 24.12 mg | 17.70 mg | 34.68 mg |
| 70 mg | 28.14 mg | 20.65 mg | 40.46 mg |
| 30 mg | 22.01 mg | ||
| 40 mg | 29.35 mg |
The conversion ratio of lisdexamfetamine dimesylate (LDX capsules) to pharmacologically active dextroamphetamine base is 0.2948.26
The conversion factor for dextroamphetamine sulfate (Attentin tablets) to dextroamphetamine base can be set at 0.7338.14
Lisdexamfetamine base is listed for informational purposes only.
1.2. L-amphetamine (L-amphetamine)
L-amphetamine (L-amphetamine) is the pure levorotatory isomer of amphetamine. Another name for it is (-)-amphetamine.
L-amphetamine is less potent than D-amphetamine with respect to dopamine transporters, while its effect on norepinephrine transporters is roughly the same.27 As a result, it has a slightly stronger noradrenergic effect than D-amphetamine, but is still predominantly dopaminergic.6
L-amphetamine raises blood pressure and heart rate more than D-amphetamine.28
The half-life of the L-enantiomer is11
- 11 hours for children ages 6 to 12
- 13 to 14 hours for adolescents aged 13 to 17
- 13 hours for adults
We are not aware of any ready-to-use L-amphetamine medication approved in Europe. It would have to be compounded in pharmacies based on an individual prescription.
1.3. Mixed amphetamine salts / amphetamine derivatives
- Adderall (U.S.): 75% dextroamphetamine and 25% levoamphetamine
* 25% each of D-amphetamine sulfate, DL-amphetamine sulfate, D-amphetamine saccharate, and DL-amphetamine aspartate monohydrate
* The various salts are metabolized at different rates, resulting in a slower rise and fall in the blood plasma concentration curve
* Immediate release: tablet with immediate release of the active ingredient
* Sustained release (Adderall® XR):
* Amphetamine salts in a capsule containing two types of pellets:
* 50% with immediate release
* 50% with an enteric coating that dissolves only in the intestine—and thus at a delayed rate—and then releases the amphetamine salt it contains
* Adderall® XR was first approved in the United States in 2001
* Crushing an Adderall® XR tablet eliminates its sustained-release effect. All of the amphetamine it contains is released immediately. - Evekeo (U.S.): 50% dextroamphetamine and 50% levoamphetamine
Amphetamine mixed salts are a combination of various stimulants:29
D-amphetamine saccharate
D-amphetamine sulfate
D,L-amphetamine sulfate
D,L-amphetamine aspartate monohydrate
While D,L-amphetamine sulfate mixtures are the most commonly used ADHD medications in the U.S., D,L-amphetamine mixtures are available in Germany only at a few pharmacies that manufacture them themselves. Production involves a wait time of several weeks. The cost was reported to be €200 for 180 capsules, each containing 5 mg of amphetamine sulfate.
1.4. Methamphetamine
- Desoxyn, USA
(1.5. Fenetyllin)
- Captagon (available in Germany until 2003; in Belgium until 2010); no longer available today
1.6. Amphetamine derivatives
There are a wide variety of amphetamine derivatives. Many are abused as drugs.
Most, but not all, amphetamine derivatives are central nervous system stimulants. Fenfluramine and p-chlorbenzphetamine have been shown to have no stimulating effect on the central nervous system.30
In this article, the terms “amphetamines” and “amphetamine-based medications” refer to medications that are still approved today and contain amphetamines as their active ingredient, which are used to treat ADHD.
1.7. History: The Discovery and Development of Amphetamine
In the 1880s, chemist Lazăr Edeleanu synthesized amphetamine for the first time. Nagai Nagayoshi was the first to isolate ephedrine from Ephedra spp., a plant used in traditional Chinese medicine, and synthesized methamphetamine for the first time in 1893.31
In the 1920s, ephedrine was sold over the counter in Europe and the United States as a decongestant and, due to its bronchodilatory and adrenaline-like effects, as a medication helpful for asthma.
In 1927, Gordon Alles synthesized racemic amphetamine and documented that it increased arousal and caused insomnia in humans and animals.
In 1935, Smith, Kline, and French Co. introduced amphetamine under the brand name Benzedrin® for the treatment of narcolepsy, postencephalitic parkinsonism, and depression.4 Benzedrin was available over the counter as a decongestant inhaler containing a cotton strip soaked in volatile amphetamine oil, which soon led to its abuse as a psychostimulant.
A few years later, Smith, Kline, and French Co. introduced the more potent dextrorotatory isomer, dextroamphetamine, under the brand name Dexedrin®.
In 1937, Charles Bradley reported on the positive effects of Benzedrine on children with behavioral problems.
In 1939, Benzedrine and Dexedrine became prescription-only drugs.
2. Approval and Prescription of Amphetamine-Based Medications
2.1. Germany
In Germany, amphetamine medications had to be prepared by pharmacists from raw materials for a long time.32 Since 2011, a D-amphetamine (Attentin) has been available in Germany as a ready-to-use medication and is approved for the treatment of ADHD (Attentin), In 2013, a D-amphetamine prodrug (lisdexamfetamine) was approved for the treatment of children. Lisdexamfetamine contains D-amphetamine in a lysine-bound form (Vyvanse). Since May 2019, Vyvanse Adult has been approved for the treatment of ADHD in adults (30, 50, 70 mg). In 2023, 20, 40, and 60 mg doses were also approved for adults. Since March 2024, Vyvanse and Vyvanse Adult have been combined into a single medication, Vyvanse, and are available in Germany in 20, 30, 40, 50, 60, and 70 mg doses.33
In Germany, lisdexamfetamine has been approved as a first-line medication for adults with ADHD since March 2024. For children and adolescents, it may still only be prescribed if MPH has proven ineffective.34353637383940
The full version of the 2017 S3 guideline, available at41 (page 72/198), noted that lisdexamfetamine could only be used in accordance with its approval following prior treatment with MPH, without limiting this statement to children.
Due to the principle of cost-effectiveness, doctors in Germany may continue to prescribe lisdexamfetamine on a health insurance prescription only if all less expensive medications (methylphenidate, specifically Medikinet rather than Ritalin for adults) have been ineffective or have caused side effects.
Lisdexamfetamine is approved in Germany for adults with no age restriction and is therefore also approved for seniors aged 60 and older. However, there are no data available on the safety and efficacy of lisdexamfetamine in people aged 60 and older. Methylphenidate and all other stimulants must be used off-label in patients aged 60 and older.42
2.2. Austria
In Austria, Vyvanse can be prescribed if other medications are ineffective or cause side effects. The doctor must provide justification for this to the health insurance provider.
2.3. Switzerland
In Switzerland, lisdexamfetamine has been marketed under the brand name Vyvanse® since 2014. Vyvanse® is approved as part of a comprehensive treatment strategy for ADHD that has persisted since childhood in children aged 6 and older, adolescents, and adults. For children aged 6 and older and adolescents, Vyvanse® may only be used if the response to prior treatment with methylphenidate is considered clinically inadequate.
Attentin® is approved in Switzerland for the treatment of ADHD in children aged six and older and adolescents up to 18 years of age as part of a comprehensive treatment strategy when the clinical response to prior treatment with methylphenidate has been inadequate.
2.4. United Kingdom
The British NICE guideline (NICE, 2018), which, like the German guideline, is regarded by experts as being highly evidence-based, explicitly recommends the use of LDX as a first-line treatment for adults with ADHD.43
2.5. USA
In the U.S., amphetamine-based medications are available as:44
- Mixture of D- and L-amphetamine isomers (racemic mixture)
- Mixed sulfates and saccharinates of D- and L-amphetamine isomers (Adderall®)
- Pure D-amphetamine sulfate
- Dexamfetamine hemisulfate (Attentin®, Amfexa®)
- D-amphetamine as lisdexamfetamine in a lysine-bound form (Vyvanse®, Tyvense®, generic versions)
- Racemic methamphetamine sulfate (Desoxyn®, USA)
In the U.S., 52.9% of adolescents with ADHD were prescribed MPH and 39.3% were prescribed amphetamine medications as their first prescription in 2018. Over the course of treatment, MPH is the primary medication prescribed for about 40% of patients, and amphetamine (AMP) is the primary medication prescribed for 33%.45
3. Effects of Amphetamine-Based Medications
Amphetamine-based medications are slightly more effective than methylphenidate46 in adults and are associated with slightly fewer side effects.
According to the current European consensus, amphetamine-based medications are the first choice of medication for ADHD in adults (ahead of methylphenidate) and the second choice of medication for children and adolescents (after methylphenidate).4748
When conducting studies on the effects of amphetamine, it is always important to keep in mind that these
- typically use AMP in significantly higher doses than is the case with ADHD medication
- Generally, use immediate release AMP / AMP that is not extended via a prodrug
- frequently inject AMP, which in turn causes it to be metabolized much more quickly
- these three factors have a synergistic effect
There is no doubt that AMP in medicinal form has a different effect than AMP in recreational form.
In terms of their chemical structure, amphetamines are closely related to the catecholamines dopamine and norepinephrine: this explains why they can bind to the receptors and transporters associated with these neurotransmitters. The great similarity among the monoamines also explains why monoamine transporters are relatively nonselective, so that the norepinephrine transporter (at least in the PFC) reuptakes more dopamine than norepinephrine.4
Source: Heal DJ, Smith SL, Gosden J, Nutt DJ (2013): Amphetamine, past and present—a pharmacological and clinical perspective. J Psychopharmacol. June 2013;27(6):479-96. doi: 10.1177/0269881113482532. PMID: 23539642; PMCID: PMC36661944, published under a Creative Commons Attribution License
Amphetamine-based medications have a more complex mechanism of action than methylphenidate.
The description of the effects of amphetamine medications is contradictory. It is sometimes argued that amphetamine medications merely inhibit dopamine reuptake and release dopamine and norepinephrine. More substantiated accounts from the United States (where amphetamine medications are prescribed more frequently than in Europe and where, as a result, they are the subject of more intensive study) cite as their effect the inhibition of dopamine and norepinephrine transporter reuptake, rather than the release of dopamine, norepinephrine, or serotonin.
In general, amphetamine-based medications are thought to act intraneuronally, while methylphenidate and atomoxetine act extraneuronally.49 Since amphetamine-based medications also target, at least in part, the dopamine transporter and the D2 autoreceptor, this view is unlikely to hold up.
AMP acts primarily in the striatum, as well as in the cortex and the ventral tegmentum.50
The first computer models capable of realistically simulating the effects of ADHD medications are now available. A computer model for simulating type 1 diabetes has already been approved by the FDA as a substitute for preclinical animal studies.51
A model for comparing MPH and AMP in children and adults with ADHD takes into account the effects on 99 proteins involved in ADHD.52
3.1. Dopamine and Amphetamine-Based Medications
The increase in dopamine levels in the PFC caused by D-amphetamine is much more pronounced and also significantly more dose-dependent than that caused by MPH, and is therefore more easily controlled.49
AMP causes:
- Extracellular dopamine levels increased 6-fold53
- tonic dopamine firing is enhanced as AMP depletes vesicular stores and promotes non-exocytotic release via reverse transport54
- Phasic dopamine firing: conflicting reports
- enhanced by upregulating vesicular dopamine release54
- Stimulants reduce phasic dopamine release53
- AMP promoted the release of dopamine from vesicles by reducing the vesicles’ affinity for dopamine uptake (from K(m) 0.8 to K(m) 32). However, the amount of dopamine released per pulse decreased by 82% (according to another source, by 25 to 50%). The D2 antagonist sulpiride reduced the inhibition of release, thereby promoting dopamine release. This release was reduced in D2-KO mice. When D2 autoreceptors were inhibited, AMP increased the amount of dopamine released into the extracellular space.55
- AMP reduces vesicular release5657 (this may affect both tonic and phasic release)
3.1.1. Effect on DAT
3.1.1.1. Dopamine reuptake inhibition via DAT and NET
Stimulants (MPH, like AMP, inhibit dopamine reuptake58 and, as a result, lead (at low doses) to a sixfold increase in extracellular dopamine levels.53
The resulting increase in extracellular dopamine levels acts on presynaptic dopamine D2 autoreceptors at the nerve terminal. Activation of the D2 autoreceptors results in a 2- to 3-fold increase in impulse-associated (phasic) dopamine release. This increase is therefore relatively smaller than the rise in extracellular dopamine. The (relatively smaller) increase in phasic dopamine acts on the postsynaptic D2 dopamine receptors and results in reduced locomotor activity. Higher doses of stimulants increase extracellular dopamine more significantly and lead to marked behavioral stimulation that cannot be overcome by the phasic activation of the inhibitory postsynaptic D2 receptors. High doses of D-AMP (drugs) cause supersaturation of extracellular postsynaptic D1 and D2 receptors, so that they outweigh the inhibitory presynaptic effect of low doses of D-AMP.53
- Amphetamine-based medications block the dopamine and norepinephrine transporters in a different way than methylphenidate. While the reuptake inhibition of MPH is similar to that of antidepressants, amphetamine-based medications act as competitive inhibitors and pseudostrata on dopamine and norepinephrine transporters and bind at the same site where the monoamines bind to the transporters, thereby also inhibiting NE and DA reuptake.59
- Amphetamine is taken up into the nerve cell via the DAT, whereas MPH is not taken up.60
- D-amphetamine is effective
- Dextroamphetamine inhibits dopamine transporters with moderate potency (Ki 34–225 nM).62
- Amphetamines can also stabilize dopamine and norepinephrine transporters in channel configurations, reverse efflux via intracellular vesicular monoamine transporters, and induce the internalization of dopamine transporters63
Doses of D-AMP result in a plasma concentration of approximately 150 nM, which is sufficient to occupy a significant proportion of the dopamine transporters. This effect is consistent with that of MPH.53 - D-amphetamine has approximately three times the affinity for norepinephrine transporters (NET) for reuptake inhibition and two and a half times the affinity for dopamine transporters (DAT) compared to racemic methylphenidate.49 Since there are barely any DATs but abundant NETs in the PFC, dopamine reuptake in the PFC occurs primarily via the NET in noradrenergic cells.4
3.1.1.1.1. DAT inhibition via PKC
- AMP may inhibit DAT via PKC64
- Several protein kinases regulate DAT function6566
- AMP increases the activity of striatal particulate PKC via a calcium-dependent signaling pathway67
- PKC activation leads to phosphorylation at the N-terminus of rat striatal DAT68
- PKC activation stimulates DAT-mediated dopamine release64
- PKC Inhibitors and the Downregulation of PKC64
- Inhibit efflux
- Do not affect dopamine uptake
3.1.1.1.2. DAT Inhibition Through DAT Internalization
AMP also leads to increased intracellular accumulation of DAT, which reduces the transport capacity for dopamine from the synaptic cleft into the cytosol.69
3.1.1.2. Increased dopamine release (DAT efflux)
Increased DAT efflux (reverse transport) increases extracellular dopamine.
Amphetamine releases dopamine from the cytosol into the extracellular space via DAT efflux.4961 58
Accordingly, amphetamines not only act as dopamine reuptake inhibitors, but they also reverse DAT function, so that the DAT not only fails to reuptake dopamine but actually releases it from the cell (efflux).70471
It is established that amphetamine-based drugs (characterized by high doses, rapid administration, and a rapid onset and offset of effects) release dopamine from the cell. However, it has not been conclusively proven that amphetamine medications (characterized by: medicinal use = low dose, slow release, long-lasting effect) also release dopamine from the cell, nor, if they do, to what extent this occurs.
Empirically, there is no doubt that amphetamine-based medications do not deplete dopamine stores, since otherwise they could not have a lasting effect.
Dopamine and norepinephrine are (re)taken up from the synaptic cleft into the nerve terminals by transporters (cytosolic pool). In the cytosol (the liquid portion of the cytoplasm), these neurotransmitters are subject to degradation, e.g., through metabolism by monoamine oxidase. To protect them from this, dopamine and norepinephrine are taken up from the cytosolic pool within the nerve terminals by VMAT2 transporters into vesicles (the vesicular pool). Vesicles that transport neurotransmitters for release are located near the cell membrane at the synaptic cleft, where, in response to electrical signals, they fuse with the cell membrane and release the neurotransmitters into the synaptic cleft (active pool in the active zone). In addition, there are vesicles located away from the cell membrane within the nerve terminal (reserve pool).
This explains why DAT efflux increases basal (tonic) extracellular dopamine while having consequences for phasic extracellular dopamine (see “Vesicular Release” below). However, there are other mechanisms through which amphetamine also increases phasic dopamine release. 4
3.1.1.2.1. Via VMAT2 at high doses
(Only) at very high doses, as a drug, amphetamines also act on the vesicular monoamine transporter 2 (VMAT2) for dopamine and norepinephrine, thereby triggering a cumulative release of dopamine from the synaptic vesicles into the cytosol.72 Subsequently, the high concentration of dopamine in the cytosol is cleared by a reversal of the dopamine transporters’ function, returning the dopamine to the synaptic cleft or the extracellular space. VMAT2 efflux is not increased at the typical dosage used for ADHD medication.8 In other words: Amphetamines at recreational doses can penetrate presynaptic monoamine vesicles and cause an efflux of neurotransmitters toward the synapse.73
A dose of 1 mg/kg of AMP (administered by injection) already caused a dopamine-DAT efflux, which was significantly higher at 10 mg/kg.74
Amphetamines in drug doses deplete the vesicles, which, as we understand it, initially leads to an increase and subsequently to a decrease in extracellular dopamine, and also impairs phasic dopamine release.
3.1.1.2.2. By increasing intracellular Ca2+
AMP increases intracellular Ca2+, which promotes the phosphorylation of DAT at the N-terminus of the transporter. Phosphorylation (by CaMKII and possibly also by PKCβ) increases the likelihood of DAT-mediated efflux of cytoplasmic DA.75
3.1.1.2.3. Increased DAT efflux via TAAR1
Amphetamine acts on DAT via TAAR1.
Amphetamine enables the trace amine-associated receptor 1 (TAAR1) to phosphorylate the DAT transporter. This blocks the reuptake of dopamine and stimulates the DAT to release dopamine (efflux).73
Dextroamphetamine ((S)-amphetamine) is the most potent TAAR1 agonist among the amphetamines.69
According to another account, stimulation of TAAR1 reduces dopamine release and, consequently, sensitivity to amphetamine.767778
3.1.2. Vesicular Release
AMP reduces vesicular release because, as a lipophilic weak base and a substrate for VMAT, it promotes the redistribution of dopamine from the synaptic vesicles into the cytosol by causing the vesicular pH gradient to collapse.56 As a result, AMP reduces the number of dopamine molecules released per vesicle.57
Amphetamine initially reduces VMAT2, while long-term administration increases it.79 MPH increases VMAT2 on its own.8081
AMP can inhibit vesicular release by indirectly activating D2 autoreceptors. The activation of D2 autoreceptors regulates potassium channels, which in turn regulate the likelihood of exocytic dopamine release.57
A computer model determined:82
- Maximum dopamine release at 0.5–1.0 mg/kg AMP (lower at lower doses than at higher doses)
- Most of the dopamine released resulted from AMP-stimulated dopamine biosynthesis
- The dopamine produced was immediately converted into DOPAC, which is secreted into the extracellular space
- The dopamine was not stored in vesicles
According to Stahl, AMP does not release dopamine, at least not at low doses.8
In both in vitro and in vivo experiments with wild-type mice, AMP caused a gradual 10-fold increase in extracellular dopamine in the striatum over approximately 30 minutes, while simultaneously reducing the dopamine pool available for electrically stimulated release. If the vesicular dopamine had previously been released into the cytosol by reserpine, extracellular dopamine did not increase; nevertheless, AMP caused a rapid rise in dopamine within 5 minutes. In DAT-KO mice, extracellular dopamine did not increase, although electrically stimulatable dopamine release was also reduced at the same time. DAT is therefore required for the dopamine-releasing effect of AMP, but not for its vesicle-emptying effect. Dopamine release from vesicles is the rate-limiting step for AMP’s effect on dopamine.83
AMP (10 microm) promoted the release of dopamine from vesicles by reducing the vesicles’ affinity for dopamine uptake (from K(m) 0.8 to K(m) 32 microm). However, the amount of dopamine released per pulse decreased by 82% (according to another source, by 25 to 50%). The D2 antagonist sulpiride reduced the inhibition of release, thereby promoting dopamine release. This release was reduced in D2-KO mice.
When D2 autoreceptors were inhibited, AMP increased the amount of dopamine released into the extracellular space.55
Depletion of vesicular DA stores through a weakly basic effect on the intravesicular pH gradient. The intravesicular pH gradient is necessary for DA concentration.
Different effects on vesicles ready for release and vesicles in the reserve pool:54
- stimulus-dependent effect in the dorsal striatum
- stimulates vesicular dopamine release
- caused by a brief fire
- via a pool of vesicles ready for release
- Reduced release
- through a long-burning fire
- that accesses the reserve pool
- These opposing effects of vesicular dopamine release were associated with a simultaneous increase in both tonic and phasic dopamine responses
- in the ventral striatum
- only increased vesicular release and increased phasic signals
3.1.3. D2 Autoreceptor Activation
In general, D-amphetamine activates D2 dopamine autoreceptors in the striatum.84
However, therapeutic doses of D-AMP do not cause a significant reduction in dopamine release via activation of D2 autoreceptors.8586
Since medications such as levodopa or piribedil do not have a positive effect on ADHD, even though one of them reduces the firing rate of dopaminergic neurons in the substantia nigra pars compacta, it is doubtful whether the reduction in hyperactivity in ADHD caused by stimulants is based on presynaptic inhibition. It is likely that the reduction in hyperkinesia caused by stimulants in ADHD is instead due to an increase in dopamine release.85
3.1.4. Increase in tyrosine hydroxylase
Amphetamine-based medications appear to have a stimulating effect on tyrosine hydroxylase in the dorsal striatum and the nucleus accumbens, leading to increased L-dopa levels; however, this does not appear to occur through a change in the phosphorylation of tyrosine hydroxylase.87
3.1.5. Increased DA firing / activation in dopaminergic brain regions
3.1.5.1. Increased DA firing in the caudate nucleus / putamen (striatum)
A high dose (significantly higher than the therapeutic dose) dose of D-amphetamine (2.5 to 10 mg/kg administered intraperitoneally in rats) leads to increased dopaminergic firing in the caudate nucleus and putamen and induces focused, repetitive (stereotypical) behavior.8889 The D2 antagonist haloperidol (2 mg/kg) terminates the excessive firing in the caudate nucleus and putamen and the reduced firing in the nucleus accumbens.88
3.1.5.2. Increased DA firing in the VTA and substantia nigra
D2 antagonists suppress increased firing in the substantia nigra and VTA (in vivo).90
3.1.5.3. Increased activation in the right orbitofrontal cortex, left middle frontal lobe, superior frontal lobe, and precentral gyrus
The improvement in ADHD symptoms following LDX treatment was accompanied by significantly increased activation in a number of brain regions that had previously been involved in reward processing under choice and feedback conditions (e.g., the left caudate and putamen, right orbitofrontal cortex, left middle frontal gyrus, superior frontal gyrus, and precentral gyrus).91
3.1.6. Reduced DA firing in the nucleus accumbens
In the nucleus accumbens, 7.5 mg/kg of D-Amp led to a reduction in dopaminergic firing.88 The D2 antagonist haloperidol (2 mg/kg) reverses the excessive firing in the caudate nucleus and putamen and the reduced firing in the nucleus accumbens.88
3.1.7. Extracellular DA in the striatum is increased to a greater extent than with MPH
In rats, amphetamine increased extracellular dopamine in the striatum by +1,400%, which is four times as much as the increase caused by MPH (+360%).92
3.1.8. AMP reduces synaptic DA binding to the same extent as MPH
In both rats and primates, amphetamine reduced synaptic dopamine binding in the striatum to the same extent as MPH (a reduction of about 25%).92
3.1.9. Indirect modulation of the DA system via effects on dopamine neurons originating in other brain regions
Amphetamine appears to influence the activity of dopamine neurons indirectly through its effects on dopamine neurons originating in other brain regions.93
Amphetamine can excite dopamine neurons by modulating glutamate neurotransmission. Amphetamine strongly inhibits the inhibitory postsynaptic potentials mediated by the metabotropic glutamate receptor (mGluR) in dopamine neurons, but has no effect on the excitatory postsynaptic currents mediated by the ionotropic glutamate receptor. Amphetamine desensitizes mGluR-mediated hyperpolarization by:94
- DA release
- Activation of postsynaptic alpha-1-adrenergic receptors
- Inhibition of InsP3-induced calcium release from internal stores
By selectively inhibiting the inhibitory component of glutamate-mediated transmission, amphetamine can promote burst firing in dopamine neurons and thereby increase the phasic release of dopamine.
3.1.10. Downregulation of dopamine receptors?
Reports of immediate downregulation of dopamine receptors following administration of amphetamine are based on studies in which rats were given amphetamine at drug doses. This applies to both the dosage (5, 10, 15 mg/kg twice daily for 4 or 20 days) and the route of administration (injection).95 Interestingly, a single dose of D-AMP actually increased the number of receptors.9586
To our knowledge, there have been no reports to date of downregulation when administered in pharmaceutical doses and formulations.
Similarly, it appears that the only studies available involve doses of amphetamines that alter dopamine receptor affinity or shift the receptor status from high-affinity to low-affinity. These doses could shift the balance between receptor statuses toward low-affinity.86
For more information on receptor status, see High-affinity and low-affinity receptor status In the article Dopamine Action at Receptors
It is conceivable, however, that amphetamine at therapeutic doses might not cause desensitization of postsynaptic or extrasynaptic (the majority of dopamine receptors are located outside synapses). However, this hypothesis has not yet been experimentally confirmed.86 It is possible that this pathway leads to the reduced psychomotor activity caused by amphetamine-based medications. In our view, however, the fact that this effect occurs as early as the first dose argues against this. On the other hand, this pathway could explain why many people with ADHD benefit from a slow, step-by-step titration of stimulants.
3.2. Norepinephrine in Amphetamine-Based Medications
While D-Amp and L-Amp increase extracellular dopamine in the PFC and striatum in a dose-dependent manner, they increase extracellular norepinephrine only in the PFC.4
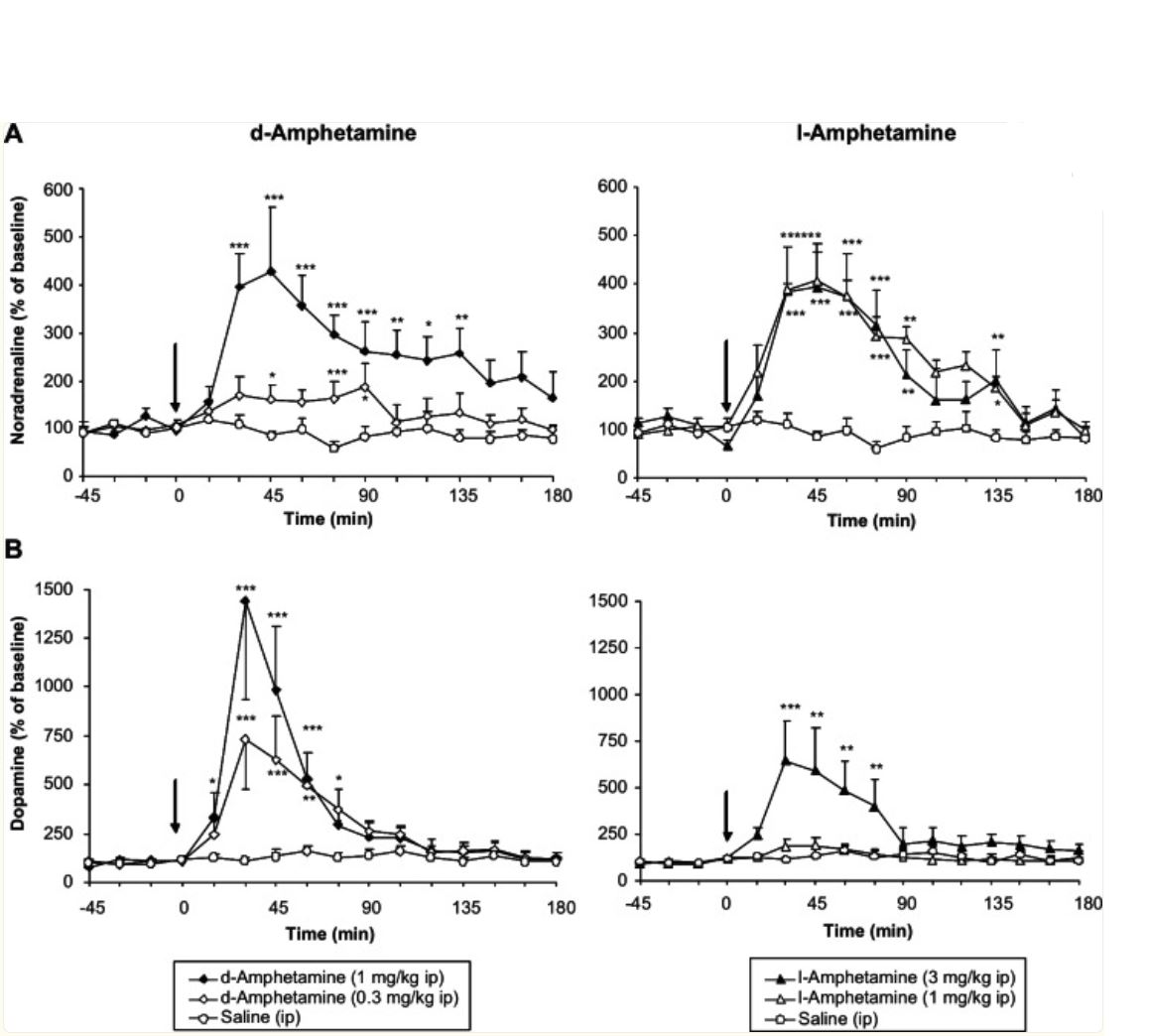
A: Extracellular norepinephrine in the PFC; dose-dependent changes induced by D-Amp and L-AMP
B: Extracellular dopamine in the striatum; dose-dependent changes induced by D-Amp and L-AMP
Source: Heal DJ, Smith SL, Gosden J, Nutt DJ (2013): Amphetamine, past and present—a pharmacological and clinical perspective. J Psychopharmacol. June 2013;27(6):479-96. doi: 10.1177/0269881113482532. PMID: 23539642; PMCID: PMC36661944, published under a Creative Commons Attribution License
3.2.1. Norepinephrine reuptake inhibition via NET
- Amphetamine-based medications block the dopamine and norepinephrine transporters in a different way than methylphenidate. While the reuptake inhibition of MPH is similar to that of antidepressants, amphetamine medications act as competitive inhibitors and pseudosubstrates at dopamine and norepinephrine transporters, binding at the same site where monoamines bind to the transporters, thereby also inhibiting the reuptake of norepinephrine and dopamine.5996
- Dextroamphetamine inhibits the norepinephrine transporter with moderate potency (Ki 39–55 nM).62
- Amphetamines can also stabilize dopamine and norepinephrine transporters in channel configurations, reverse efflux via intracellular vesicular monoamine transporters, and induce the internalization of dopamine transporters.63
- D-amphetamine has approximately one-third the inhibitory effect on norepinephrine transporters (NET) and dopamine transporters (DAT) as racemic methylphenidate.49
- Amphetamine (as well as ephedrine) also inhibits the intracellular norepinephrine transporter, which takes up norepinephrine from the nerve cell into the vesicles (the neurotransmitter storage sites)96
3.2.2. Norepinephrine release
- Whether amphetamine in medicinal doses stimulates the release of norepinephrine is a subject of debate, just as it is with dopamine. There are arguments both against8 and in favor of this.5861
- D-amphetamine indirectly increases the release of norepinephrine.84 This is always the case with dopaminergic medications due to the conversion of dopamine (at a rate of approximately 5 to 10%) into norepinephrine.
- There is no doubt that amphetamine medications do not lead to a chronic depletion of norepinephrine stores in the sense of a deficiency. It has been empirically established that amphetamine medications for ADHD do not cause any tolerance effects, even over the long term.
In mice, 2.5 mg/kg of AMP caused:97
- stereotypical behavior (a sign of a sharp increase in extracellular dopamine); as pronounced as with 20 mg/kg MPH
- Increased extracellular dopamine
- Increased extracellular norepinephrine
- Increased extracellular serotonin
3.2.3. Reduction in norepinephrine metabolites only in responders
- Several independent studies have found that D-amphetamine medications reduce levels of MHPG, a metabolite of norepinephrine, in urine. The decrease in MHPG in urine is said to be an important indicator of the onset of stimulant effects, suggesting a reduction in norepinephrine levels caused by dextroamphetamine medications.98](https://psycnet.apa.org/psycinfo/1982-21744-001)
- Furthermore, the reduction in norepinephrine metabolites occurs only in people with ADHD who respond positively to dexamfetamine (responders).99
- Similarly, when methylphenidate was administered, only the responders showed a significant decrease in urinary MPHG, while urinary MPHG levels did not decrease in the nonresponders.100
The authors conclude that this indicates reduced norepinephrine levels in ADHD. - Furthermore, several studies involving people with ADHD found that behavioral improvements were proportional to the reduction in the level of the norepinephrine metabolite norepinephrine (achieved through the use of dextroamphetamine).101
In contrast to the reduction in urinary metabolites caused by D-amphetamine, the D-amphetamine-induced increase in norepinephrine in the PFC is roughly as pronounced as that caused by MPH, but is significantly more dose-dependent and therefore more easily controlled.49
3.2.4. Increased DA firing and DA bursting via norepinephrine α1 receptors
D-Amp (1 to 2 mg/kg) increases dopaminergic firing and bursting in the substantia nigra and VTA (in vivo) via alpha-1 adrenoceptors102 (but not via alpha-2 or beta adrenoceptors). This adrenergic pathway is normally masked by the reduction in dopaminergic firing mediated by D2 autoreceptors and becomes apparent with the use of D2 antagonists or the concurrent administration of D1/D5 and D2/D3/D4 blockers. The selective norepinephrine reuptake inhibitor nisoxetine did not increase the DA firing rate, but it did increase DA bursts.90103
D-amphetamine appears to activate the norepinephrine α1 receptor in the PFC, as the α1 receptor antagonist prazosin completely neutralized the effects of D-amphetamine in the PFC. In contrast, D-amphetamine does not appear to act on either the α2 receptor or the β receptor, as the effects of D-amphetamine persisted even when the α2 or β receptors were blocked.104
D-amphetamine promotes the “up” state of cortical neurons by activating105
- Central α1A-adrenoceptors
- D1 receptors
- D2 receptors
- But not through D1 or D2 receptors alone, respectively
In contrast, L-DOPA, a precursor to dopamine and norepinephrine, did not promote the “up” state.
Arousal is associated with an elevated “Up” state, while slow-wave sleep, general anesthesia, and a calm waking state are characterized by an oscillating alternation between “Up” and “Down” states. During arousal, the “down” states end, and the “up/down” oscillation transitions into a sustained “up” state.
The up/down oscillations appear to be relevant to memory consolidation, while the transition to a sustained up state is necessary for arousal and attention.105
3.3. Adrenaline
Peripherally, amphetamine triggers the release of neurotransmitters from the sympathetic nervous system, which explains its cardiovascular side effects.4
3.4. Monoamine
3.4.1. Inhibition of monoamine breakdown via MAO
Amphetamine-based medications act—albeit rather weakly4 —as MAO inhibitors,10650 unlike low-dose MPH. It is unknown whether high-dose MPH acts as an MAO inhibitor.49
MAO is an enzyme that breaks down dopamine and norepinephrine within the cell. MAO inhibitors therefore increase the amount of dopamine and norepinephrine available within the cell. Since dopamine and norepinephrine continue to be synthesized within the nerve cell, the levels of norepinephrine and dopamine in the cell continue to rise. This reverses the action of the transporters (which normally return DA and NE from the synaptic cleft back into the cell), causing them to release NE and DA into the synaptic cleft even without being triggered by a nerve signal that needs to be transmitted.106 This effect triggers peripheral hypertension and an increase in heart rate. Since this mechanism of action occurs indirectly at the presynapse, ephedrine and amphetamine-based medications are also called “indirect sympathomimetics,” whereas active ingredients that act directly on the receptors at the postsynapse are called sympathomimetics.106
3.4.2. Monoamine Release
Dextroamphetamine increases monoamine release from presynaptic terminals107, possibly through an interaction with the vesicular monoamine transporter 2 and the reversal of plasma membrane monoamine transporters.62
3.5. Serotonin
3.5.1. Serotonin reuptake inhibition
Dextroamphetamine also inhibits serotonin transporters to a small extent (Ki 1.4–3.8 μM).107
3.5.2. Serotonin release
Amphetamine medications are said to release small amounts of serotonin.1085 Here, too, it is unclear whether this is actually the case at therapeutic doses or whether this effect is limited to recreational drug use. In any case, Stahl does not report any serotonergic effects of amphetamine medications.59
In mice, 2.5 mg/kg of AMP caused:97
- stereotypical behavior (a sign of a sharp increase in extracellular dopamine); as pronounced as with 20 mg/kg MPH
- Increased extracellular dopamine
- Increased extracellular norepinephrine
- Increased extracellular serotonin
Serotonin Release Induced by Amphetamine Drugs
Amphetamine-type drugs (MDMA, MBDB) also increase serotonin release. It is believed that amphetamine-induced serotonin release not only influences psychomotor activation but also affects subjective well-being (and, when taken as a drug, euphoria as well).109 MDBD causes almost no dopamine release.
Hyperactivity induced by 5 mg or 10 mg/kg of MDMA (= a dosage 10 to 20 times higher than that used for medical purposes) was prevented by prior administration of 2.5 and 10 mg/kg of the selective serotonin reuptake inhibitor fluoxetine. Fluoxetine had the same effect with regard to the interactive effects of MDMA and p-chloroamphetamine.110 This suggests that MDMA causes hyperactivity by increasing serotonin levels via the serotonin transporter, which was blocked by fluoxetine as a serotonin reuptake inhibitor.
- There is evidence that increased serotonin release indirectly raises dopamine levels.110
- Other sources suggest that amphetamine salts have a serotonin-enhancing effect due to their inhibition of monoamine oxidase.10
- Amphetamine increases c-Fos expression in the mPFC, striatum, and nucleus accumbens. A serotonin 1A receptor agonist reduced the increase in c-Fos in the mPFC and striatum, but not in the nucleus accumbens.111
- MPH itself acts as an agonist at the 5-HT1A receptor.50
3.6. Effect on the HPA axis
3.6.1. Elevated ACTH
Lisdexamfetamine and d-amphetamine significantly increased plasma ACTH levels in healthy individuals.112
3.6.2. Increased corticosteroids
- D-amphetamine medications such as lisdexamfetamine (Vyvanse) increase cortisol levels but do not increase testosterone levels.112
- The following were increased:
- Glucocorticoids (such as methylphenidate; the increase was even greater with the drugs MDMA or LSD)
- Cortisol
- Cortisone
- Corticosterone
- 11-Dehydrocorticosterone,
- 11-Deoxycortisol
- Glucocorticoids (such as methylphenidate; the increase was even greater with the drugs MDMA or LSD)
- The following remained unchanged
- Mineralocorticoids
- Aldosterone
- 11-Deoxycorticosterone
- Mineralocorticoids
The increase in cortisol levels causes cortisol to bind more strongly to the glucocorticoid receptor (GR). Through the GR, cortisol triggers the deactivation of the HPA axis at the end of the stress response.
In ADHD-HI and ADHD-C (both of which involve hyperactivity), it is reasonable to assume that, due to the blunted endocrine stress response of the adrenal glands, the GRs are not sufficiently activated to shut down the HPA axis following a stress response. Furthermore, in ADHD-HI (unlike in ADHD-I), there is often impaired GR function, which further complicates the deactivation of the HPA axis.
For more information, see “Medications for ADHD” at ⇒ Dexamethasone for ADHD. If AMP increases cortisol release, this could improve the downregulation of the HPA axis in ADHD-HI. However, since AMP is also effective in ADHD-I, the primary mechanism of action is likely to be different.
3.6.3. Increased levels of steroid hormones
In healthy subjects, lisdexamfetamine and d-amphetamine significantly increased plasma levels of, among others:112
- Androgens
- Dehydroepiandrosterone
- Dehydroepiandrosterone sulfate
- Androstenedione (Δ4-androsten-3,17-dione)
- Progesterone (for men only)
The androgen remained unchanged
- Testosterone
Since aggression correlates with an elevated testosterone-to-cortisol ratio, amphetamine medications have an aggression-inhibiting effect due to the relative increase in cortisol levels.
For more information, visit ⇒ Neurophysiological Correlates of Aggression
A study of adolescent rhesus monkeys found as a consequence of 12 months of treatment with AMP or MPH at therapeutic doses that both active ingredients increased testosterone levels, with MPH having a more pronounced effect than AMP.113 Another study in rhesus monkeys found reduced testosterone levels following MPH administration.114
In rodents, a decrease in testosterone levels has been observed following administration of amphetamine.115116
3.7. Inhibition of OCT2
Fundamentals of Uptake-2 Transporters under Dopamine Degradation by Organic Cation Transporters (OCT) In the article Dopamine Reuptake, Dopamine Degradation
The organic cation transporter 2 (OCT2) plays a role in the breakdown of dopamine. OCTs take up dopamine, norepinephrine, serotonin, and—to a slightly greater extent—histamine into glial cells, where they are broken down by COMT. OCT2 and OCT3 are also located on (including dopaminergic) neurons.
While methylphenidate binds only to OCT1 (IC50: 0.36) and not to OCT2, OCT3, or PMAT117, d-amphetamine acts as a highly potent hOCT2 reuptake inhibitor (Ki: 10.5 mM) and a moderately potent hOCT1 reuptake inhibitor (Ki: 202 mM), while it did not interact with hOCT3 until concentrations of 100 μM or higher (Ki: 460 mM) (hOCT: human OCT).117118
d-amphetamine binds with approximately the same affinity to hOCT2 and hOCT3, and with an affinity that is one order of magnitude (a factor of 10) weaker than that for DAT.118
The binding of amphetamine to OCT may contribute to the cellular and behavioral effects of amphetamine.118
OCT2 reuptake inhibitors have antidepressant effects.119 Furthermore, in OCT2-KO mice, much lower doses of venlafaxine or reboxetine have antidepressant effects than in wild-type mice.120
We believe it is worth considering whether this approach might also support the effects of dopamine reuptake inhibitors in ADHD.
Furthermore, these correlations could explain why AMP, which also acts as an OCT2 inhibitor, has a greater antidepressant effect than MPH, which binds only to OCT1.
3.8. Other Effects on Brain Functions
- D-amphetamine increases metabolism in the right caudate nucleus and decreases it in the right Rolandi region as well as in the right anterior inferior frontal regions.121
- Neuroprotective effects in stroke or traumatic brain injury
- D-amphetamine (as well as L-dopa, which, however, has no effect whatsoever on ADHD despite its dopaminergic action) is also suitable for restoring brain function after strokes, but only if appropriate training measures are implemented at the same time.122 D-amphetamine increases dopamine, which has a neurotrophic effect (promoting neuroplasticity). Dopaminergic medications such as (D-)amphetamine-based drugs or MPH can therefore also support appropriate training measures (e.g., neurofeedback, cognitive behavioral therapy) in ADHD by reducing limitations in learning ability.
- Low-dose methamphetamine administered within 12 hours of a stroke or traumatic brain injury had a neuroprotective effect and improved cognitive function and functional behavior.123
- There are similar reports regarding MPH, although in that case as well, rapid administration following a traumatic brain injury appears to be key124
- Methylphenidate and amphetamine-based medications increase alpha activity (in rats), while atomoxetine and guanfacine do not.125
- Lisdexamfetamine (Vyvanse) causes126
- Elevated acetylcholine levels in the cortex
- Elevated histamine levels in the cortex and hippocampus (which concurrent escitalopram treatment prevents only in the hippocampus)
Amphetamine-based medications are therefore not merely a substitute for methylphenidate, but have their own specific indications.
3.9. Overview of AMP and Neurotransmitters
3.9.1. Binding Affinity of AMP, MPH, and ATX to DAT, NET, and SERT
The active ingredients methylphenidate (MPH), d-amphetamine (d-AMP), l-amphetamine (l-AMP), and atomoxetine (ATX) bind with varying affinities to the dopamine transporter (DAT), norepinephrine transporter (NET), and serotonin transporter (SERT). This binding inhibits the activity of the respective transporters.127
The values reported by Easton et al. in the following table refer to levels in the synaptosome, as well as to DAT in the striatum and NET in the PFC.
| Binding affinity: higher for smaller numbers (KD = Ki) | DAT | NET | SERT |
|---|---|---|---|
| MPH | 34 - 200127 , 3416 | 2386, 339127 | > 10,000127 |
| d-AMP (Vyvanse, Attentin) | 34–41127 , 206 (sulfate) 6 | ** 23.3–38.9**127 , 54.8 (sulfate)6 | 3,830–11,000127 |
| l-AMP | 138127 , 1435 (sulfate) 6 | ** 30.1**127 , 259 (sulfate)6 | 57,000127 |
| ATX | 1451 - 1600127 23556 | ** 2.6 - 5**127 , 20.66 | ** 48 - 77**127 |
| GBR-12909 | 40.26 | ||
| Desipramine | 4.96 |
3.9.2. Effects of AMP, MPH, and ATX on Dopamine and Norepinephrine by Brain Region
The active ingredients methylphenidate (MPH), amphetamine (AMP), and atomoxetine (ATX) affect extracellular dopamine (DA) and norepinephrine (NE) to varying degrees in different regions of the brain. Table modified from Madras,127.
| PFC | ; striatum | ; nucleus accumbens | |
|---|---|---|---|
| MPH | DA + NE (+) |
DA + NE +/- 0 |
DA + NE +/- 0 |
| AMP | DA + NE + |
DA + NE +/- 0 |
DA + NE +/- 0 |
| ATX | DA + NE + |
DA +/- 0 NE +/- 0 |
DA +/- 0 NE +/- 0 |
4. Effects of Amphetamine-Based Medications Compared to MPH / Atomoxetine
In a randomized, double-blind study involving n = 200 participants, lisdexamfetamine (EU: Vyvanse) was compared with atomoxetine in patients who did not respond to MPH. Lisdexamfetamine performed significantly better than atomoxetine in 2 of 6 categories and in the overall assessment.128
In a double-blind study, lisdexamfetamine (EU: Vyvanse) was also effective in treating comorbid symptoms of depression.129 MPH is not known to have any positive effects on symptoms of depression.
A 2-year study of children and adolescents (n = 314) showed a response rate of between 70 and 77%, with good efficacy and manageable side effects.130
5. Effect on ADHD Symptoms
For people with ADHD who respond positively to D-amphetamine medications as well as to MPH, the effectiveness of D-amphetamine medications is at least equal to that of MPH131; in our experience with adults, it is even significantly better.
For a comparison of the effectiveness of individual medications and treatment methods, see ⇒ Effect sizes of various ADHD treatments.
According to the current European consensus, amphetamine-based medications are the first-line choice of medication for ADHD in adults (ahead of methylphenidate) and the second-line choice of medication for children (after methylphenidate).4748
Amphetamine-based medications should also always be tried when MPH is ineffective (non-responders).
5.1. ADHD-I (without hyperactivity)
For most people with ADHD, MPH has a more stimulating effect and boosts motivation more than AMP-based medications. Contrary reports132 do not align with our experience.
We are also unable to confirm, based on our experience, the claims made in the professional literature that amphetamine-based medications are more suitable for people with ADHD-I than MPH—in part because people with ADHD-I are disproportionately likely to be non-responders to MPH—133 .
We know quite a few people with ADHD-HI who respond significantly better to amphetamine medications than to MPH, as well as people with ADHD-I who do better on MPH. Based on our observations, we cannot identify any subtype-specific effects of amphetamine medications or methylphenidate. In our experience, amphetamine medications are just as effective for ADHD-HI as they are for ADHD-I.
5.2. Attention Control
People with ADHD have reduced extrinsic and intrinsic motivation. For example, they need greater rewards to be just as motivated to do something as people without ADHD. However, once motivation is sparked in people with ADHD, their attention and its controllability can no longer be reliably distinguished from that of people without ADHD. ⇒ A shift in motivation toward one’s own needs explains regulatory problems
Attention correlates, among other things, with a deactivation of the default mode network (DMN). Stimulants are capable of bringing the attention control of people with ADHD (or their level of motivation, from which attention follows) in line with that of people without ADHD, which is then also reflected in a normalization of DMN deactivation.134
For more information on the altered functioning of the DMN in ADHD and its normalization through stimulants, including additional references, visit ⇒ DMN (Default Mode Network) In the article ⇒ Neurophysiological Correlates of Hyperactivity.
The references cited pertain to the effects of methylphenidate. However, it can be assumed that these effects are generally produced by stimulants.
People with ADHD report that MPH allows for greater focus, while amphetamine-based medications (Vyvanse) tend to promote a more relaxed state of general alertness and feel somewhat more pleasant overall.
5.3. Comorbid Depression or Dysthymia
Amphetamine-based medications also appear to have a mild serotonergic effect and are therefore particularly useful in cases of comorbid dysthymia or depression, especially since selective serotonin reuptake inhibitors (SSRIs) can have adverse effects in ADHD (particularly in ADHD-I) (see the relevant section).
In online forums, many people with ADHD report that amphetamine-based medications have a significant antidepressant effect, which they do not experience with MPH.135 This is consistent with the experiences of users known to us.
Since amphetamines can have a more potent stimulating effect than MPH, this may trigger an existing suicidal tendency that had not previously been acted upon due to the underlying depression. Amphetamine medications should therefore be used with caution in cases of severe depression (including undiagnosed depression).
Note: A suspected case of dysthymia (mild chronic depression) in people with ADHD must be clearly distinguished from the primary ADHD symptom of dysphoria during inactivity.
For more information, visit ⇒ Depression and Dysphoria in ADHD In the section ⇒ Differential Diagnosis of ADHD.
5.4. Co-occurring Anxiety Disorders / Depression
Comorbid anxiety disorders or depression may be exacerbated by stimulants, as anxiety and mood are regulated by dopaminergic activity in the ventromedial prefrontal cortex (PFC) in conjunction with the limbic system.59
5.5. Comorbid Sleep Disorders
Amphetamine-based medications have a fairly long duration of action (up to 13 hours). Taking them too late (less than 14 hours before bedtime) could therefore cause difficulty falling asleep. Some people with ADHD report feeling pleasantly drowsy in the evening when taking amphetamine medications and say they no longer have trouble falling asleep.
Studies show that amphetamine-based medications improve overall sleep quality in people with ADHD.136137
5.6. Impulsivity
People with ADHD have reported on forums that MPH is more effective at reducing impulsivity than Vyvanse (lisdexamfetamine).138
6. Response Rate (Responding / Nonresponding)
“Response” here refers to whether a positive effect on ADHD symptoms can be observed. People with ADHD who do not respond adequately to a medication are called nonresponders.
“Nonresponsive” does not mean that there is no effect, but simply that the effect falls short of the level of symptom improvement defined in the respective study.
A study reports a response rate of 80% (defined as an improvement of more than 30% in ADHD-RS-IV scores and markedly or very markedly improved CGI-I ratings).139
A summary of several studies reports a 69% response rate to amphetamine-based medications and a 59% response rate to methylphenidate. 87% of people with ADHD reportedly responded to one of the two types of active ingredients.2
A 2-year study of levamphetamine medications in children and adolescents (n = 314) showed a response rate of between 70 and 77%, with good efficacy and manageable side effects.130
For MPH non-responders, it is therefore highly recommended to try treatment with amphetamine-based medications (see 1.2.), and vice versa.
According to a Cochrane study, all amphetamine-based medications are equally effective in adults.140 Since the studies analyzed in the Cochrane meta-analysis did not examine the effects of LDX and dAMP in the same individuals, the meta-analysis can only provide information about the statistical response rates of the various active ingredients themselves, and nothing about whether different amphetamine-based medications work differently well for people with ADHD.
There are reports that dextroamphetamine sulfate (without the lysine moiety) may be effective for some people with ADHD in whom LDX did not work (well) or took too long to take effect. This is also noted in an information sheet that describes the factors to consider when switching from LDX to dAMP.141
In addition, there are an increasing number of reports from clinical practice that different lisdexamfetamine formulations may (but by no means necessarily) exhibit significant intra-individual differences. This is true even for people with ADHD who had not previously considered the possibility that such differences might exist, or who were convinced that these were completely interchangeable products. Some people with ADHD reported that they were able to reliably reproduce differences in effect by alternating between different formulations on a daily basis. There is no pharmacological explanation for this.
In individuals with the COMT Val-158-Met gene polymorphism, amphetamine increases PFC efficiency in subjects with presumably low dopamine levels in the PFC. In contrast, in individuals with the COMT Met-158-Met polymorphism, amphetamine had no effect on cortical efficiency under low- to moderate-level working memory load and caused a decline under high working memory load. Individuals with the Met-158-Met polymorphism appear to have an increased risk of an adverse reaction to amphetamine.142
In practice, it has not yet been possible to predict how a person will respond. A study of preschool children in the United States found that white children responded better to stimulants (MPH, lisdexamfetamine) than children of color; other factors (age, gender) had no effect.143
People with ADHD for whom ADHD medications were ineffective (nonresponders) reported higher levels of trauma on the Perceived Stress Scale (PSS) than people with ADHD for whom medications were effective (responders).144
Among those not affected, the number of traumatic childhood events correlated with the level of currently experienced stress, as well as with a stronger dopamine response in the ventral striatum to amphetamine.145
This could be an indication that increased childhood trauma is associated with an increased striatal dopamine response to stimulants, suggesting that a significantly lower dose of stimulants would be more appropriate for these people with ADHD. We can immediately think of people with ADHD for whom this is true.
7. No gender-specific differences in efficacy
Amphetamine-based medications do not appear to show any gender-specific differences in their effects.146
8. At low doses, it has a calming effect; at high doses, it has a stimulating effect
D-amphetamine appears to have a biphasic effect profile. Low (pharmaceutical) doses of 0.5 to 1 mg/kg in rats (corresponding to approximately 0.2 to 0.6 mg/kg in humans) reduce (hyper)activity, while higher (drug) doses increase it.53
It is possible that amphetamines do not always increase dopamine levels, but rather, under certain circumstances, have a dopamine-normalizing effect.
Bmal1-cKO mice exhibited increased dopamine release, increased excitability of striatal neurons, and ADGS symptoms such as hyperactivity, attention problems, and working memory deficits. Amphetamine and the D1 receptor antagonist SCH23390 reduced hyperactivity.147
9. Dosage of Amphetamine Medications or MPH
About 66% of all people with ADHD respond equally well to MPH and to amphetamine-based medications.
22% respond better to amphetamine-based medications than to MPH.
11% respond better to MPH than to amphetamine-based medications.148
About 15% of people with ADHD respond best to the active ingredient D-amphetamine.149
Based on these findings, it would make more sense to first try treatment with amphetamine-based medications and only consider MPH as a second option if the patient does not respond to them, since people with ADHD respond slightly better to amphetamine-based medications than to MPH.
Highly gifted individuals with ADHD (here: IQ > 120) are said to respond better to amphetamine-based medications than less gifted individuals with ADHD.150
An interesting study examines the effectiveness of lisdexamfetamine.151
It is recommended to start with a very low dose and increase it gradually. Even if the optimal dose were known, starting with the optimal dose right away could potentially be too much for the body to handle.152 The symptoms of ADHD arise from signal transmission problems between the brain’s neurons because neurotransmitter levels (dopamine, norepinephrine) are too low. Optimal neurotransmitter levels resolve these signal transmission problems. If neurotransmitter levels are too high due to an overdose, signal transmission is disrupted just as much as when levels are too low.
This explains why treatment should begin with a low dose and then, with persistent effort, be gradually increased until a worsening of symptoms is observed.
Since the number of dopamine transporters in adults is half that of 10-year-olds, it is advisable to start with a much lower dose than that used for children.
10. Efficacy Profile (Over Time) / Duration of Effect
In replicated studies on the duration of action of amphetamine medications, children had a shorter half-life of approximately 7 hours, while adults had a longer half-life of approximately 10 to 12 hours.153
The temporal course of the effect (effect profile) depends less on the active ingredients than on the specific composition of the medication.
Vyvanse has a very prolonged dose-response profile without pronounced peaks, so that onset and rebound effects are barely noticeable. See: Graphical representation of the Vyvanse pharmacokinetic profile. However, the graph, which is taken from Shire’s patent application, refers to plasma levels in rats at an extremely high dose of 3 mg/kg.
Another graph shows the drug concentration profiles for 30 mg, 50 mg, and 70 mg of Vyvanse, on page 20.
It remains unclear to what extent the binding of D-amphetamine to lysine in lisdexamfetamine actually results in a flatter and prolonged concentration of amphetamine in blood plasma. A single dose of 40 mg of D-amphetamine (exceeding medically appropriate doses) or 100 mg of lisdexamfetamine administered to healthy individuals showed no significant differences in plasma amphetamine concentrations.154 Furthermore, the study data appear to indicate a subjective impression among the participants that lisdexamfetamine has a gentler and longer-lasting effect, although the authors do not report this. Another limitation of the study is that the participants were treated with a single dose, and no titration to the tested dosage was performed. The authors themselves cite studies indicating that amphetamine medications require a titration phase or exhibit (initial) habituation effects. The study’s results are therefore primarily of pharmacological interest but are of limited practical value.
Empirically, adults report quite unanimously that lisdexamfetamine has a gentler and longer-lasting effect. The majority cite a duration of action of 5 to 7 hours for a single dose. There is also a fairly unanimous report of a very delayed onset of action, with 1 to 2 hours most commonly cited.
An internal (and non-representative) survey on adhs-forum.adx.org regarding the duration of Vyvanse’s effects (n = 80), as well as another survey in a Vyvanse subreddit (n = 467), yielded the following results (n = 547):
| Duration of action of a single dose of Vyvanse | % of participants |
|---|---|
| 5 hours or less | 40.8% |
| 6 to 7 hours | 26.7% |
| 8 to 9 hours | , 15.4% |
| 10 to 11 hours | , 11% |
| 12 hours or more | , 6.2% |
The surveys are not representative (they do not take age, weight, dosage, or gender into account), but they clearly show that a duration of action of 13 or 14 hours, as stated by the manufacturer, is achieved in adults only in exceptional cases, if at all.
A more detailed survey on the duration of effect of a single dose of all ADHD medications—which also takes the aforementioned secondary factors into account—has been underway since March 2023 and could yield initial results in the fall of 2023.
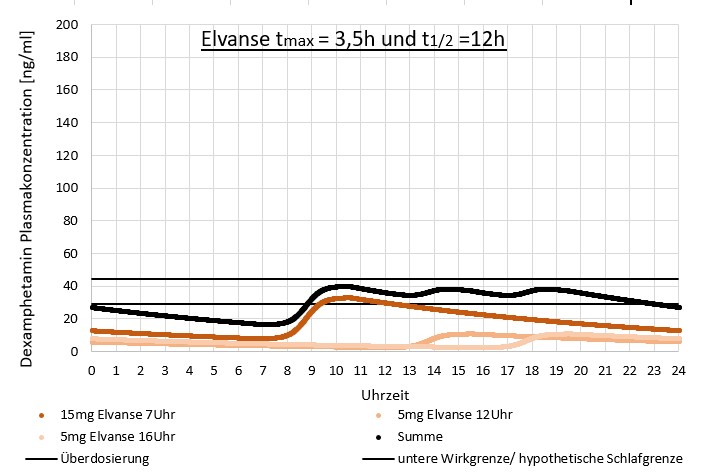
Many people with ADHD (we know of countless cases from the forum) take 2 or 3 single doses of Vyvanse per day to achieve the necessary all-day coverage, even though this does not comply with the manufacturer’s guidelines. The individually shortened duration of action could also be a consequence of a low dosage—often 30 mg or less per single dose—which was chosen when an overdose was perceived at a higher single dose during the phase of high D-AMP blood plasma levels. For almost none of the people with ADHD does the total of the single doses exceed 70 mg per day.
The effect of taking multiple small doses of Vyvanse on D-AMP blood plasma levels could (purely hypothetically) look like this:
11. Uses of amphetamine-based medications compared to MPH
According to the current European consensus on the diagnosis and treatment of ADHD in adults, amphetamine-based medications are the first-line choice of medication for ADHD in adults (ahead of methylphenidate) and the second-line choice of medication for children (after methylphenidate).4748
For children who are MPH nonresponders—that is, who do not respond to MPH—the effectiveness of amphetamine medications should be evaluated.
People with severe dysphoria when inactive or with comorbid depression benefit particularly from amphetamine medications.
In addition, people with ADHD who need a greater boost of energy may find that amphetamine-based medications work better for them.
Highly gifted individuals are said to respond better to amphetamine-based medications than to MPH.150
12. Side Effects
An analysis of reports submitted to the WHO VigiAccess database revealed the following relative frequency of adverse event reports for dextroamphetamine (the percentages do not indicate the frequency of occurrence during use):155
| Report Rate % | Side Effects |
|---|---|
| 4.3% | Unexpected therapeutic reaction |
| 3.08% | : Headaches |
| 1.96% | Depressive Mood |
| 1.86% | Fatigue |
| 1.74% | Insomnia |
| 1.68% | Nausea |
| 1.67% | Heart Palpitations |
| 1.64% | Attention Disorders |
| 1.43% | Anxiety |
| 1.35% | Dizziness |
| 1.16% | Drowsiness |
| 1.15% | Loss of appetite |
| 1.13% | Irritability |
| 1.03% | Feeling unwell |
| 0.94% | Unrest |
| 0.9% | Dry mouth |
| 0.83% | Aggressiveness |
| 0.8% | Excitement |
4.84% of the reports concerned a lack of efficacy of the medication, and 1.75% concerned a problem with product substitution.
The analysis does not distinguish between sustained release and immediate release AMP or AMP in prodrug form (lisdexamfetamine). Sustained release and prodrug medications have a lower incidence of side effects.
12.1. No liver damage at standard drug dosages
High doses of amphetamines may be associated with liver damage and certain forms of clinically apparent liver damage. This is most commonly reported with methylenedioxymethamphetamine (MDMA: “Ecstasy”).156
Amphetamine-based medications, on the other hand, are prescribed at such low doses that this does not occur: It’s the dose that makes the poison. See also ⇒ Stimulants as Medications Versus Stimulants as Drugs.
12.2. AMP increases histamine levels only in the central nervous system
AMP centrally increases histamine,157158 just like all other known ADHD medications:
- Atomoxetine
- Methylphenidate
- Modafinil
- Nicotine
- Caffeine
However, this increase in the central nervous system does not affect the body; therefore, ADHD medications do not raise histamine levels in the body and should not cause any problems for people with histamine intolerance.
However, people with ADHD and histamine intolerance reported that they could not tolerate AMP or sustained-release MPH at all, but were able to tolerate immediate-release MPH in small doses.
12.3. No increased cardiovascular risks
Several large studies found no increased risk of serious cardiovascular events—such as stroke, heart attack, or cardiac arrhythmias—associated with amphetamine-based medications.159160
A 14-year study found a 4% increase in the risk of cardiovascular problems for each year of use of stimulants (methylphenidate, amphetamine-based medications) and, to a slightly lesser extent, the non-stimulant atomoxetine.161
According to a meta-analysis, daily use of amphetamine-based medications resulted in:162
- systolic blood pressure increased by 1.93 mmHg (k = 56 RCTs, n = 10,583)
- diastolic blood pressure increased by 1.84 mmHg (k = 56 RCTs, n = 10,583)
- Heart rate increased by 3.71 beats per minute (k = 47 RCTs, n = 10,075)
12.4. Individual Cases of Trichotillomania
There have been reports of isolated cases of trichotillomania (hair pulling).163 Trichotillomania is a specific type of impulse control disorder.
12.5. Erection, Libido, Reproduction
The Vyvanse package insert lists erectile dysfunction as occurring in 1 to 10 out of 100 men. However, the scientific literature and studies do not report any sexual side effects caused by amphetamine-based medications.
Posts on the ADxS ADHD forum occasionally mention erectile problems associated with amphetamine-based medications, but barely with MPH.
Two male people with ADHD reported a loss of sensitivity in the genital area after consuming red wine outside the active period of their regularly taken Vyvanse. In one of the people with ADHD, low nicotine consumption outside the active period is another factor raising suspicion.
A case report documents a decrease in testosterone and other sex hormones, as well as a decrease in sperm count, caused by an amphetamine medication; this was resolved by switching back to MPH.164
Amphetamine-based medications also bind to alpha-1 adrenoreceptors (see above).
Blockade of alpha-1 adrenoceptors leads to delayed detumescence of the corpora cavernosa and thus to a reduced ability to ejaculate and achieve orgasm in both women and men.165 Blockade is the opposite of binding. Dopamine agonists such as L-dopa or bromocriptine increase sexual desire and sexual activity.
Amphetamines (typically when used as a drug) can alter spermatogenesis and lead to oxidative stress and subsequent apoptosis in testicular tissue.166
Amphetamine in a therapeutic dose (in this case, lisdexamfetamine) did not alter testosterone levels.167
In rodents, amphetamine (at pharmacological doses) can reduce testosterone production and increase the formation of cyclic AMP in the testes.166
A single intravenous injection of amphetamine (administered as a drug) reduced hCG-stimulated testosterone release. Plasma LH levels remained unchanged.
Amphetamine thus appears to have a direct, dose-dependent effect on Leydig cells, where it inhibits testosterone production by activating adenylate cyclase.115
A single intraperitoneal dose of methamphetamine initially lowered serum testosterone levels but increased them after 48 hours to a level above the baseline.168
Chronic high-dose methamphetamine administration reduced testosterone169 and increased GABA in the testes.170 GABA is involved in Leydig cell proliferation and testosterone production.
MDMA inhibits the hypothalamic-pituitary-gonadal axis in male rats. Both acute and chronic MDMA administration resulted in reduced serum testosterone and decreased GnRH mRNA expression. LH, progesterone, and estradiol remained unchanged. This suggests that reduced drive from hypothalamic GnRH neurons is the cause of the inhibition of the hypothalamic-pituitary-gonadal axis.171
Subcutaneous administration of MDMA for 12 weeks on three consecutive days per week (which simulated weekend use in humans) did not alter the hormones of the hypothalamic-pituitary-gonadal axis.172
Methamphetamine can trigger apoptosis in mouse testicular germ cells173174 and reduce sperm count.175
Rats that received 5 ml/kg of methamphetamine intraperitoneally for 7 and 14 days (drug dose) showed a significantly reduced number of spermatogonia, primary and secondary spermatocytes, as well as spermatogenesis indices (tubule differentiation index, spermatogenesis index, repopulation index, and mean diameter of the testicular tubules).176
MDMA is also capable of inducing histological changes in the testes of rats and causing dose-dependent DNA damage to sperm. However, sperm count increased while spermatid count decreased.172 MDMA increased body temperature and the immunoreactivity of heat shock protein 70 (HSP70), which could trigger apoptosis in rat testicular tissue.177
A pilot study of men with sexual problems reports improvements in subjective sexual experience (shorter time to orgasm or increased frequency of orgasm) following administration of 5 to 20 mg of amphetamine salts (Adderall) taken 1 to 4 hours before sexual activity (up to 10 doses per month).178
In 5 individual cases, the resolution of SSRI-induced sexual dysfunction was reported following low doses of dextroamphetamine or methylphenidate.179 Other case studies report multiple erections (in a 15-year-old), hypersexual behavior (in an 8-year-old) caused by OROS-MPH (Concerta)180, and priapism (in a 14-year-old).181
A study reports a twofold increase in the rate of testosterone deficiency among adults with ADHD after 5 years of stimulant use (1.2%) compared to people with ADHD who do not take stimulants (0.67%) or people without ADHD (0.68%).182
12.6. Amphetamine-Based Medications for Older Adults
There are only a few studies on the efficacy and safety of amphetamine-based medications in older adults.
A study found no increased risks associated with lisdexamfetamine in people aged 55 to 84. No age-related trends were observed in changes in heart rate or blood pressure, and the safety profile of LDX was identical to that observed in younger adult study participants. The clearance of LDX decreased with age, so a lower dose is recommended, and a prolonged effect is to be expected.183
This is consistent with our experience regarding stimulants in older adults with ADHD. Nevertheless, particularly careful monitoring of blood pressure changes is recommended.
12.7. Miscellaneous
Common side effects of amphetamine mixed salts include:29
- Loss of appetite
- Mood swings
Rare serious side effects of amphetamine mixed salts include:29
- psychotic symptoms
- Seizures
- Risk of misuse
The drug MDMA (unlike amphetamine-based medications) can damage nerve cells and compromise the blood-brain barrier.184
12.8. Overdose
Symptoms of a (severe) amphetamine overdose (in the sense of poisoning) include, among others:
- Agitation185
- Hyperactivity186
- Movement disorders185
- Tremor185
- Hyperthermia186
- Tachycardia (rapid heartbeat)186
- Tachypnea (increased respiratory rate)186
- Mydriasis (dilated pupils)186185
- Tremors186
- Seizures186, which in extreme cases can progress to epileptic forms185
- Hyperreflexia (excessive reflex response)185
- combative behavior185
- Confusion185
- Hallucinations185
- Delirium185
- Anxiety185
- Paranoia185
It is hardly surprising that doses of 11.3 mg/kg of LDX cause toxic effects in rats, since this is significantly higher than therapeutic doses.187
13. Metabolism of Amphetamine
13.1. Breakdown of LDX to d-AMP
Lisdexamfetamine (Vyvanse) is converted to d-AMP in the erythrocyte cytosol by an unknown amino acid (presumably an aminopeptidase)188189 through the cleavage of the covalent bond between d-amphetamine and L-lysine. Only d-AMP is pharmacologically active. d-AMP is primarily eliminated renally; the remainder is presumably metabolized via CYP2D6.
96% of LDX is excreted in the urine; of this21
- 42% of the dose as AMP
- 25% as hippuric acid
- 2% as intact LDX.
Unlike AMP, LDX is not very sensitive to changes in urine pH.
The half-life of LDX is typically less than 1 hour.
13.2. Breakdown of D-AMP and L-AMP
Dextroamphetamine is said to have a half-life of
- about 7 hours190
- 9–11 hours
Taking it with a high-fat meal can extend the half-life of d-AMP by one hour.
A half-life of 11–14 hours has been reported for l-Amp.
Two online surveys of a combined total of approximately 550 people with ADHD who take lisdexamfetamine showed that about 40% experience a duration of action of 5 hours or less per single dose, and two-thirds experience a duration of action of 7 hours or less per single dose. For more information, see Effects and Duration of ADHD Medications
Some amphetamine is excreted unchanged in the urine. This depends on the body’s pH level, with which the (easily measurable) urine pH level correlates. When the urine pH is acidic, a large amount of amphetamine is excreted unchanged (up to over 50%); when the urine pH is alkaline, this figure drops to less than 5%.
The remaining amphetamine is metabolized through various pathways.
Phase 1 Metabolism of Amphetamine
- Catalysis by cytochrome P450 and flavin monooxygenase
- 4-hydroxyamphetamine (active metabolite formed by aromatic hydroxylation)
- Metabolism to 4-hydroxy-norephedrine
- Alpha-hydroxyamphetamine
- Demineralization via 2YP2D6
- possibly deamination to phenylacetone (P2P) via a presumed carbinolamine intermediate191
- Metabolism to benzoic acid
- direct glucuronidation to benzoic acid
- or, first, oxidation to a hydroxyketo analog, which is then converted to benzoic acid191
- subsequent oxidation of benzoic acid at the benzyl position to p-hydroxynorephedrine (according to some sources, via dopamine beta-hydroxylase)
- Breakdown into hippuric acid (glycine conjugate)
- Metabolism to benzoic acid
- Norephedrine (phenylpropanolamine) (active metabolite)
- Metabolism to 4-hydroxy-norephedrine
Alternatively:
- Direct oxidation of amphetamine by dopamine beta-hydroxylase to norephedrine191
Alternatively:
- N-Hydroxylation of amphetamine and related derivatives191
- The N-hydroxy derivatives can be further oxidized to nitroso, nitro, and oximino compounds.
- The oximino derivative could be hydrolyzed to phenylacetone (so far, this has only been described theoretically)
- Other metabolites are possible
Phase 2 Reactions:191
- Conjugation of ring-hydroxylated metabolites to their corresponding glucuronides
- Sulfation of the enol form of phenylacetone
13.2.1. Primary route of elimination: renal, acid-dependent
Some of the AMP is excreted unchanged by the kidneys before it can exert a pharmacological effect centrally. It exerts its effect peripherally even before that.
Since AMP is slightly basic (pKA = 9.9), AMP excretion depends heavily on the pH of the urine and the flow rate, with AMP recovery in the urine ranging from 1% to 75% and the remainder being metabolized by the liver:21
- normal urine pH levels21
- 30 to 40% of the AMP dose is excreted largely as the unchanged parent compound
- 50% of the dose is excreted as alpha-hydroxyamphetamine or its downstream inactive metabolite, hippuric acid
- acidic urine
- alkaline urine
The half-life of AMP is expected to increase by 7 hours for each unit increase in pH. However, this is likely to depend on the initial pH value. Acidifying or alkalizing agents can therefore significantly alter the effect of AMP.
For more information, see Acid-Base Balance and Amphetamine Medications In the article “ : Potency and Duration of Action of ADHD Medications”.
13.2.2. Secondary metabolic pathway: CYP2D6, CYP1A2, and CYP3A4
According to recent publications, the portion of amphetamine that is not metabolized by the kidneys is broken down via aromatic hydroxylation by CYP2D6, CYP1A2, and CYP3A4.113
The extent to which this breakdown of amphetamine by CYP450 is medically relevant in humans is a matter of debate. Most studies have been conducted in vitro or in vivo in rats.
According to other sources, d-amphetamine is metabolized without the involvement of CYP.193
13.2.2.1. Metabolism of amphetamine by CYP3A4
CYP3A4 is described as an additional, secondary metabolic pathway for dextroamphetamine.194
13.2.2.2. Metabolism of amphetamine by CYP2D6
There are very few studies on the metabolism of amphetamine-based medications via CYP2D6 in humans.
A study found that CYP2D6 poor metabolizers were 3.67 times more likely to show symptom improvement than CYP2D6 intermediate metabolizers (after adjusting for phenotype conversion and controlling for sex, age, dose, duration, and adherence). Self-reported side effects were not influenced by the CYP2D6 metabolism phenotype.195
A study of n = 15,000 participants found that the CYP2D6 gene had a clinically relevant effect on amphetamine metabolism in 5% (Supplement Table 2) to 6% (text) of the participants.196
Another study found no statistically significant effect of CYP2D6 metabolism type on dextroamphetamine or lisdexamfetamine, which may have been due to the small sample size.197 The smaller the sample size, the more pronounced the effect must be to be statistically significant.
These results suggest that CYP2D6 plays a medically significant role in the metabolism of amphetamine-based medications in humans. However, further studies are needed to obtain reliable findings.
For comparison: CYP2D6 poor metabolizers had atomoxetine levels up to ten times higher than normal metabolizers at comparable doses. ATX is primarily metabolized via CYP2D6.198
The clinical literature assumes that amphetamine is metabolized by CYP2D6, without going into further detail or identifying other metabolic pathways.
199200201
The FDA warns CYP2D6 poor metabolizers about potential problems with amphetamine-based medications.202 Stahl’s Essential Prescriber’s Guide203 identifies amphetamine as a substrate of CYP2D6. Feder et al. (2023) identify CYP2D6 as the primary metabolic pathway for dextroamphetamine in the Child Medication Fact Book for Psychiatric Practice.204
The EUR Research Information Portal notes “only” a known interaction between amphetamine and clonidine, which is metabolized via CYP2D6.205
The Adderall product information mentions that the drug may be metabolized by CYP2D6 and warns of changes in efficacy caused by CYP2D6 inhibitors.206
Until studies are available that provide specific dosing recommendations, physicians should at least consider the realistic possibility that CYP2D6 inhibitors may increase amphetamine levels, which is equivalent to a dose increase.207
The scientific literature on ADHD draws conclusions solely from in vitro laboratory studies on human cells or from in vivo laboratory studies on rodents:
According to most sources, dextroamphetamine is metabolized by CYP2D6189208 , at least to a small extent209
Numerous sources take it for granted that amphetamine is metabolized by CYP2D6, without further questioning this assumption.210211
Others conclude that poor CYP2D6 metabolizers likely require lower doses of AMP, while ultra-rapid metabolizers likely require higher doses of AMP. However, they further note that the effects of CYP2D6 polymorphisms on AMP metabolism remain unclear15321 212 , so the extent to which the CYP2D6 genotype influences the efficacy of amphetamine medications for ADHD is still unclear.213
Although CYP2D6 is involved in the metabolism of d-AMP, it is not the dominant metabolic pathway.214
The further the scientific literature moves away from the practical application of amphetamine as a medication in humans, the smaller the assumed contribution of CYP2D6 to the metabolism of amphetamine becomes. It should be noted that these studies were not only conducted predominantly on rodents rather than humans, but also often focused more on the metabolism of amphetamine at drug doses than on the metabolism of the comparatively low medicinal doses:
Amphetamine itself appears to be metabolized by CYP2D6 to a much lesser extent than some amphetamine analogs.215216 In vivo, CYP2D6 appears to play a smaller role in the metabolism of amphetamines than it does in vitro.217
Neither amphetamine (AM, beta-phenylisopropylamine) nor the amphetamine derivatives N-ethylamfetamine (NEA), N-butylamfetamine (NBA), 4-methoxyamphetamine (M-AM), 4-methoxy-N-ethylamfetamine (M-NEA), or 4-methoxy-N-butylamfetamine (M-NBA) were N-dealkylated to any significant extent in microsomal, human, CYP2D6-expressing cell preparations. The only metabolites formed from AM, NEA, and NBA were the corresponding 4-hydroxylated compounds, whose formation rates were low. All 4-methoxylated substrates were efficiently O-demethylated by CYP2D6 to their corresponding phenols. The size of the N-alkyl group influenced the formation rates of these phenolamines. In contrast to the reported results with 2- and 3-methoxyamphetamines, none of the 4-methoxyamphetamines were ring-oxidized in the CYP2D6 enzyme system to 2- or 3-hydroxy-4-methoxyamfetamines or dihydroxyamfetamines in the CYP2D6 enzyme system.215
The N,N-dialkylated amphetamine, N-methyl-N-propargylamfetamine (deprenyl; DEP), was N-demethylated and N-depropargylated by CYP2D6. N-benzyl-N-methylamphetamine (benzphetamine; BPA), on the other hand, did not form any metabolites via CYP2D6. N-allyl-N-methylamphetamine (AMA), N,N-diallylamphetamine (DAA), and N-methyl-N-propylamfetamine (MPA) underwent CYP2D6-catalyzed N-dealkylation. The rates of CYP2D6-catalyzed reactions on N,N-dialkylated amphetamines depended on the type and degree of unsaturation of the N-substituents.218
In rats and rabbits, amphetamine and six amphetamine derivatives showed that amphetamine itself had the highest affinity (lowest K_m) for CYP2C3, and that an increase in the size of the substituent on the nitrogen atom reduced the affinity. The reaction rate increased with the size of the substituent. The rates of N-demethylation of BZP and deprenyl by rat CYP2C11 and 2C13 were far higher than those of reactions at other N-alpha positions. This suggests that rat CYP2C enzymes exhibit stricter regioselectivity than rabbit CYP2C3 for the deamination/N-dealkylation of phenylisopropylamines.219
In rats, a CYP2D1 inhibitor led to an increased or prolonged effect of AMP and a doubling of AMP’s AUC.220 CYP2D1 in rats corresponds to human CYP2D6 .
Metabolism of amphetamine-type drugs by CYP
The metabolism of methamphetamine (N-methyl-alpha-methylphenethylamine, crystal meth) has been studied most frequently.
Methamphetamine (Crystal Meth)
CYP2D6 has been identified as the primary metabolic pathway for methamphetamine, whereas MDMA is not oxidized by CYP2D6.221 In addition, there is evidence that methamphetamine interacts with CYP2C6 as well as the CYP2D family.222 Ethanol was shown to influence methamphetamine metabolism via CYP3A and CYP2E1.223
Studies using human liver microsomes, including those involving CYP2D6 slow metabolizers, provided evidence of a significant role for CYP2D6 in the aromatic 4-hydroxylation of methamphetamine. The rate of the 4-hydroxylation reaction was significantly slower than the demethylation of MDMA (ecstasy).221
Methamphetamine binds to CYP3A4 in two ways, both of which result in N-demethylation, with K_D values of 0.016 ± 0.001 and 204 ± 18 μM, respectively.224
Excretion of methamphetamine:191
- approx. 23% unchanged
- 18% as p-hydroxymethamphetamine
- 14% as the demethylated product
MDMA (Ecstasy): Research findings are contradictory.
- Human
- Demethylation:
- N-dealkylation:
- In humans, MDMA is metabolized primarily by CYP2D6. At the same time, MDMA is a potent CYP2D6 inhibitor.227
- Rat
MDMB
- Human
- Rat
The catalytic N-demethylation of MBDB in rats and humans was primarily mediated by CYP1A2 and, to a lesser extent, by CYP2D1 in rats or polymorphic CYP2D6 in humans. MBDB was also N-demethylated by CYP3A2/4.226
MDA
MDE
- Human
- Rat
BDB
The catalytic N-deethylation of MDE in rats and humans was primarily mediated by CYP3A2/4; in rats, it was also mediated to a small extent by CYP1A2 and CYP2D1.226
Designer drugs derived from amphetamines have two important, overlapping metabolic pathways:
- O-demethylation to dihydroxy derivatives (catechols)225228
- Methylation of one of the hydroxy groups and glucuronidation or sulfation, followed by gradual degradation of the side chain to N-dealkyl and deaminooxo metabolites225228
In addition, there are other degradation pathways, such as
- aromatic hydroxylation225
- Phase I oxidative metabolism, usually catalyzed by cytochrome P450 enzymes (e.g., CYP2D6, CYP2C19). In this process, a hydrogen atom on the aromatic ring is replaced by an OH group. Through this process, amphetamine is metabolized to p-hydroxyamphetamine.
- The propylamines MDA (methylenedioxyamphetamine), MDMA, and MDE (methylenedioxyethylamphetamine) are metabolized not only as glycine conjugates of the corresponding 3,4-disubstituted benzoic acids—known as hippuric acid derivatives—which could occur via COMT-catalyzed methylation and/or glucuronidation/sulfation229
The CYP2D6 polymorphism does not appear to account for the large interindividual differences in the toxicity of designer drugs that have been observed empirically.228 The catalytic demethylation of MDA, MDMA, MDE, BDB, and MBDB to catechols in humans and rats was primarily mediated by CYP2D1, CYP2D6, CYP3A2, and CYP3A4; in humans, the demethylation of MDMA and MBDB was additionally mediated by CYP1A2.226
13.2.2.3. Inhibition of CYP2D6 by amphetamine
Amphetamine is a potent CYP2D6 inhibitor.216 A CYP2D6 inhibitor blocks the activity of CYP2D6, causing other medications metabolized by CYP2D6 to be broken down more slowly, which can quickly lead to an overdose.
The CYP2D6 gene is highly polymorphic. The alleles of particular relevance in Central Europe are230
- CYP2D6*3
- CYP2D6*4
- CYP2D6*5
- CYP2D6*6
- CYP2D6*9
- CYP2D6*41
Based on experience with the influence of CYP2D6 on the effects of other medications (CYP2D6 is responsible for the metabolism of 20–30% of all medications), the various CYP2D6 gene variants result in different metabolism types:230
- Slow metabolizers - approx. 7%
- It is important to add the dose very slowly
- A particularly low dosage is helpful
- Moderately fast metabolizers - approx. 40%
- Fast metabolizers - about 46%
- Ultra-fast metabolizers - approx. 7%
- CYP2D6*XN allele
- increased enzyme activity
- is associated with treatment resistance (non-responders)
- An increased dose may be helpful
For more information, see –> CYP2D6 Metabolizing Enzyme
Anecdotal reports:
- On the ADxS forum, several people with ADHD reported a significant prolongation of the duration of action of a single dose of an amphetamine medication due to berberine, which is metabolized by CYP2D6 and CYP3A4 and is therefore a competitor for these enzymes. Similarly, bupropion prolongs the effects of amphetamine-based medications. Bupropion is a potent CYP2D6 inhibitor and is not affected by CYP3A4.
- We were also informed of a case of serotonin syndrome and severe side effects that occurred when paroxetine was administered in addition to lisdexamfetamine. Paroxetine is metabolized by CYP2D6 and is itself a potent inhibitor of CYP2D6. In the reported case, both medications had to be discontinued immediately as an emergency measure within 2 days.
Until more robust research data are available, the precautionary principle should be applied when prescribing amphetamine-based medications, and metabolism by or interaction with CYP2D6 should at least be considered.
13.2.3. Flavin Monooxygenase Degradation Pathway
Flavin monooxygenase (FMO3) is a monooxygenase system similar to CYP.
FMO oxidizes secondary and tertiary amine analogs of amphetamine.191
(+/-)-Amphetamine hydroxylamine is converted by human FMO3 to phenylpropanone oxime with a trans/cis stereoselectivity ratio of 5:1. Methamphetamine is oxidized by human FMO3 at the N-position to methamphetamine hydroxylamine.231
Flavin-containing monooxygenases (FMOs) oxidize drugs and xenobiotics that contain a “soft nucleophile,” typically nitrogen or sulfur. Although FMOs have a lesser influence than CYP on the oxidative metabolism of xenobiotics, their role is not negligible.232
- FMOs, like CYP, are monooxygenases and exhibit similar tissue and cellular localization, molecular weight, and substrate specificity
- There are 5 FMO families, each with one member. Unlike CYP, FMO does not require a reductase to transfer electrons from NADPH and exhibits a catalytic cycle that is significantly different from that of CYP
- Unlike CYP, FMOs cannot be induced by xenobiotics
- The substrates of FMO and CYP overlap, but often result in different metabolites with potentially significant toxicological/pharmacological Consequences
- Three of the five expressed human FMO genes—FMO1, FMO2, and FMO3—exhibit genetic polymorphisms
- FMO3 in the adult liver has been studied most extensively
- A defect in the FMO3 allele causes the disorder trimethylaminuria
In addition, FMOs are involved in the breakdown of232
- ABT418 (selective agonist for neuronal nicotinic acetylcholine receptors): FMO1 (pig)
- Amitriptyline: FMO1 pig, Km 100
- Benzphetamines: FMO1 (pig), Km 74
- Chlorimipramine: FMO1 pig, Km 40
- Chlorpromazine: FMO1 pig, Km 9
- Clozapine: human FMO3, K_m 324
- Desipramine: FMO1 pig, Km 250
- Ephedrine: FMO1 pig
- Imipramine: FMO1 in pigs, Km 22; also in humans
- Nicotine
- (S)-nicotine: FMO2 monkey, Km 1700; also human
- (R)-(+)-nicotine: FMO1 (pig), Km 70
- Nortryptiline: FMO1 pig, Km 500
- Promazin: FMO1 Pig, Km 66
- Prometazin: FMO1 Pig, Km 120
- Propranolol: FMO1 pig, Km 210
- Tamoxifen: Human FMO3, Km 1200
- Tyramine: Human FMO3, Km 220–950
13.2.4. Dopamine-beta-hydroxylase degradation pathway
Dextroamphetamine, but not levoamphetamine, is metabolized by dopamine β-hydroxylase (DBH). DBH catalyzes the removal of the pro-R hydrogen atom and the formation of 1-norephedrine, (2S,1R)-2-amino-1-hydroxy-1-phenylpropane, from d-amphetamine.233
Amphetamine also appears to be broken down by dopamine beta-hydroxylase.234235
However, this is contradicted by the fact that, although pretreatment with a dopamine β-hydroxylase inhibitor prior to amphetamine administration led to a reduction in amphetamine metabolites, it did not alter the level of amphetamine in the brain.236
13.2.5. Methylation (dAMP to methamphetamine)
A laboratory study found evidence that medical dextroamphetamine is metabolized to methamphetamine via N-methylation in humans in vivo. 31% of the urine samples contained dextromethamphetamine, albeit at levels below 1%. Metabolism via this pathway therefore occurs in such small quantities that it is likely medically irrelevant; however, it is significant for the detection of amphetamine when drug use is suspected. No methamphetamine was detected during the in vitro metabolism of lisdexamfetamine or dextroamphetamine (neither dMeth nor lMeth). Among methamphetamine drugs, a racemic mixture of levo- and dextromethamphetamine was not typically found; instead, the vast majority consisted of pure lMeth or dMeth.237238
The propylamines MDA (methylenedioxyamphetamine), MDMA, and MDE (methylenedioxyethylamfetamine) are metabolized not only as glycine conjugates of the corresponding 3,4-disubstituted benzoic acids—the so-called hippuric acid derivatives—which could occur via COMT-catalyzed methylation and/or glucuronidation/sulfation229
For more on AMP drugs vs. AMP medications in the lab, see also Drug Tests and ADHD Medications
14. Contraindications and Drug Interactions
As with any medication described here, there are also contraindications for amphetamine-based medications.
Do not take this medication without first consulting a doctor.
- Pregnancy / Breastfeeding
- No adverse effects on the child were observed when the mother continued taking D-Amp during pregnancy. In contrast, discontinuing D-Amp use during pregnancy was associated with an increased risk of miscarriage. Benefits were observed when D-Amp was not taken before or during pregnancy. Therefore, discontinuing use in a timely manner may be helpful for women planning to conceive.239
- A cohort study found no increased risk of ADHD or other neurodevelopmental disorders associated with taking MPH or AMP during pregnancy.240
- Risk of neurodevelopmental disorders in children remains unchanged with ATX use during pregnancy (Swedish cohort study, n = 861,650 children of n = 572,731 mothers from 2008 to 2017)241
- CYP Development in Fetuses, Newborns, and Infants242
- Fetal liver microsomes exhibit only 1% of the CYP2D6 activity seen in adults.
- Within a month after birth, this value rises to about 20% of an adult’s activity level.
- The immaturity of the CYP2D6 system at birth could explain the syndrome characterized by irritability, tachypnea, tremor, and increased muscle tone in newborns whose mothers took SSRIs, provided that it is not, alternatively, a withdrawal reaction to the SSRI.
- In our opinion, if this is relevant, women should refrain from taking amphetamine-based medications during pregnancy until it is clarified whether these medications are metabolized by CYP2D6.
- By age 3, CYP metabolism is well developed
- Children have a proportionally larger amount of liver parenchyma than adults, so weight-adjusted metabolic capacity is greater in childhood
- The immaturity of the CYP2D6 system at birth could explain the syndrome characterized by irritability, tachypnea, tremor, and increased muscle tone in newborns whose mothers took SSRIs, provided that it is not, alternatively, a withdrawal reaction to the SSRI.
- Weight of Newborns
- Unchanged, among mothers with ADHD who took amphetamine medications during pregnancy.243 This is consistent with the findings of a large cohort study on the use of MPH during pregnancy.244
- a slight decrease in birth weight and a slight increase in the risk of preeclampsia, placental abruption, or preterm birth when taking stimulants (AMP or MPH) during pregnancy; however, these increases were so small that the authors did not recommend discontinuing stimulant use during pregnancy.245 Atomoxetine did not show these slight increases in risk.
- Miscarriages
- The risk of miscarriage doubles when taking stimulants during pregnancy.246
- Malformations
For lisdexamfetamine:249
- Hypersensitivity to the active ingredient
- Monoamine oxidase inhibitors (MAOIs) taken at the same time or within 14 days prior to taking this medication
- Risk: hypertensive crisis
- Hyperthyroidism / Thyrotoxicosis
- States of arousal
- Symptomatic cardiovascular disease
- Advanced atherosclerosis
- Moderate to severe hypertension
- Glaucoma
- Serotonin reuptake inhibitors
- When SSRIs and amphetamine-based medications are administered concurrently, the risk of serotonin syndrome should be taken into account.10
According to a very large study, the risk of developing psychosis among people with ADHD who take MPH is 0.10%, which is lower than that of those treated with amphetamine-based medications (0.21%).250 While people with ADHD treated with stimulants have 2.4 cases of psychosis per 1,000 person-years, the rate for the general population is 0.214%.251 The studies do not allow for a conclusion as to whether the increased prevalence of psychosis is attributable to ADHD or to stimulants.
The studies do not allow us to conclude whether the increase in the prevalence of psychosis is attributable to the presence of ADHD or to the use of stimulants.
Another study found an 8-fold increased risk among people with ADHD who were taking ADHD medication (0.34% vs. 0.048%).252 Since this study compares people with ADHD who are taking medication—rather than those with and without medication—to the general population, no reliable conclusions can be drawn about the role of ADHD medications. The absolute risk of a first-time episode of psychosis or mania upon starting medication was dependent on the active ingredient:
- Atomoxetine: 0.60% (highest)
- Amphetamine-based medications: 0.33%
- Methylphenidate: 0.19%
14.1. Shorter half-life (reduced effect)
Dexamfetamine’s effects are reduced by:253
- Adrenoreceptor blockers (beta blockers)
- e.g.:
- Propranolol
- e.g.:
- Lithium
- Phenothiazines
- Haloperidol
- Substances that lower the pH level in the gastrointestinal tract
- e.g.:
- Guanethidine
- Reserpine
- Glutamic acid
- Hydrochloric acid
- Ascorbic acid
- Fruit juice
- result in reduced absorption of dexamfetamine
- e.g.:
- Substances that acidify urine (ammonium chloride, sodium dihydrogen phosphate, etc.)
- increase the levels of ionized dexamfetamine metabolites in urine, leading to an increase in renal excretio
- When urine becomes acidic (lower pH)249
e.g., by- Ascorbic acid
- Thiazide diuretics
- High-protein diet
- Diabetes mellitus
Note: Foods that taste sour often have an alkalizing effect in the body beyond the digestive tract.
Example: Lemon juice has a pH of 2.4 and therefore has an acidic effect on the mouth and stomach. After digestion, however, only alkaline residues remain in the rest of the body, which raise the pH.
The effect of foods, after digestion, on the acid load on the kidneys due to minerals and protein is indicated by the PRAL value (potential renal acid load). This value is not suitable for assessing the acid load on the mouth and stomach (as is relevant in cases of heartburn).
The higher the PRAL value, the more acidic the effect on the kidneys and the rest of the body beyond the digestive organs.
Urine pH has proven to be a good marker of PRAL. An alkaline urine pH correlates with a diet that has a negative PRAL value, while urine pH levels below 6.0 correlate with an acid-forming diet.
It is important to distinguish between plant-based and animal-based proteins. After 7 days on a vegetarian diet, the urine pH rises and the PRAL value decreases; the same occurs with a vegetarian diet for 2 or 3 days per week.254 A vegetarian diet is thus associated with a prolonged effect of amphetamine-based medications.
Foods high in oxalate can increase acid production.255
A study provides the following calculation formula:256 PRAL (mEq/d) = 0.49 × Protein (g/d) + 0.037 × Phosphorus (mg/d) − 0.021 × Potassium (mg/d) - 0.026 × magnesium (mg/d) - 0.013 × calcium (mg/d).
In other words: Foods with a strongly negative PRAL value result in alkaline (less acidic) urine and thus promote a prolonged effect of amphetamine medications. Foods with a high PRAL value result in acidic urine and thus promote a shorter duration of action for amphetamine medications. According to this model, hard cheese is suitable for shortening the duration of action of amphetamine medications, while raisins could prolong it.
For more information, see Acid-Base Balance and Amphetamine Medications In the article Effects and Duration of ADHD Medications
14.2. Extended half-life (increased effect)
- In cases of alkaline urine (elevated pH):249
e.g., by- Sodium bicarbonate (baking powder, soda)
- A diet high in fruits and vegetables
- Urinary Tract Infections
- Vomiting
- Clonidine253
Enhanced effects of dexamfetamine due to:253
- Disulfiram
- Substances that raise the pH level in the gastrointestinal tract increase dexamfetamine absorption
- e.g.:
- Sodium bicarbonate (baking soda)
- e.g.:
- Substances that increase the pH of urine increase the levels of non-ionized metabolites in the urine, which reduces renal excretion and thus increases blood levels of dexamfetamine
- e.g.:
- Acetazolamide
- some thiazides
- e.g.:
There is evidence that reduced expression of the CACNA1C gene may lead to a prolonged effect of dopamine reuptake inhibitors.257 Conversely, increased CACNA1C expression is likely to result in a shorter duration of action.
14.3. Delayed effect
When taken with a high-fat meal, lisdexamfetamine (Vyvanse) reaches its peak blood level one hour later (4.7 hours instead of 3.8 hours after administration).258 However, other parameters, such as the duration of action, remain unchanged.
14.4. Potentiating effect on amphetamines
14.4.1. Alcohol increases amphetamine levels
Alcohol can increase amphetamine levels.207
14.4.2. CYP2D6 inhibitors increase amphetamine levels
Since amphetamine is metabolized by CYP2D6, medications that are also metabolized by CYP2D6 can slow down both the metabolism of amphetamine and their own metabolism, as this creates competition for the CYP2D6 enzyme.
CYP2D6 inhibitors can increase amphetamine levels, making a dose reduction necessary. After discontinuing CYP2D6 inhibitors, an increase in the dose of amphetamine medications may be necessary.207
CYP2D6 inducers can accelerate metabolism and thus reduce the effect.
A study found that lisdexamfetamine had no effect on CYP2D6, CYP1A2, or CYP3A.259
For more information, see CYP2D6 Metabolizing Enzyme
14.5. Attenuating effect on amphetamines
The following have an attenuating effect on amphetamine:260
- Chlorpromazine
- Haloperidol
- Lithium carbonate
One person with ADHD told us that Vyvanse became less effective when taken with 2 mg of dienogest (Zafrilla) for endometriosis, while the effectiveness of Attentin remained unchanged.
14.6. AMP has few interactions with other medications
In contrast to the interactions between amphetamine medications and other drugs mentioned above, there are barely any known interactions between amphetamine medications and other drugs.207
Amphetamines can increase serotonin release and inhibit serotonin reuptake. Therefore, taking amphetamines and SSRIs at the same time carries the risk of dangerously high extracellular serotonin levels (serotonin syndrome).213261
We are aware of such cases, for example, involving the concurrent use of lisdexamfetamine and the SSRI paroxetine.
Amphetamine is said to have a slight inhibitory effect on cytochromes
- CYP2D6
- CYP1A2
- CYP3A4.
The clinical relevance is considered to be low.260
Attenuating effect on260
- Antihypertensive drugs, such as guanethidine
Reinforcing260
- Analgesic effect of opioids
14.7. AMP During Pregnancy
A small prospective study of n = 13 children whose mothers received amphetamine medications while breastfeeding found no adverse effects on the children.262
15. Long-term effects: No tolerance to amphetamine medications
A meta-analysis of 87 randomized, placebo-controlled, double-blind studies found no evidence of a decline in the efficacy of methylphenidate, amphetamine-based medications, atomoxetine, or α2-antagonists with long-term use.263
16. Preparations
Amphetamine medications are available in various forms.
In the U.S., amphetamine-based medications are available as:44
- Mixture of D- and L-amphetamine isomers (racemic mixture)
- Mixed sulfates and saccharinates of D-L-amphetamine isomers (Adderall)
- Pure D-amphetamine sulfate
- Dexamfetamine hemisulfate
- United Kingdom: Amfexa®
- Germany, Denmark, Finland, Iceland, Luxembourg, Norway, Sweden: Attentin®
- Approved for children and adolescents ages 6 to 17
- Packages: 5 mg tablets, 10 mg breakable tablets
- Dosage: 5–10 mg/day orally, with an increase of 5 mg per week, up to a maximum dose of 20 mg/day (up to 40 mg for older children in exceptional cases)264
- Dexamfetamine hemisulfate
- D-amphetamine as lisdexamfetamine in a lysine-bound form (Vyvanse, Tyvense)
- Racemic methamphetamine sulfate (Desoxyn)
Vyvanse, Tyvense
Vyvanse / Tyvense contains lisdexamfetamine. Lisdexamfetamine is dextroamphetamine bound to lysine. The lysine bond results in a very slow and steady release of dextroamphetamine into the bloodstream, thereby prolonging its effect.
- United States (“Vyvanse”)
- Hard capsules
- Early 2007: 30, 50, 70 mg
- End of 2007: 20, 30, 40, 50, 60, 70 mg
- 2014: 10, 20, 30, 40, 50, 60, 70 mg
- Many older studies (particularly clinical trials) therefore examined only 30 mg, 50 mg, and 70 mg.
- Chewable tablets
- 20 mg, 30 mg, 40 mg, 50 mg, 60 mg, 70 mg
- Hard capsules
- Canada
- 10 mg, 20 mg, 30 mg, 40 mg, 50 mg, 60 mg, 70 mg
- United Kingdom
- Vyvanse will be available in two dosage forms containing the same active ingredient through 2024
- Vyvanse (approved for children, 2013); 20, 30, 40, 50, 60, 70 mg
- Vyvanse for adults (approved for adults)
- May 2019: 30, 50, 70 mg
- 2023: 20, 30, 40, 50, 60 mg, 70 mg
- In 2024, the marketing authorizations for Vyvanse and Vyvanse Adult were consolidated, so that only Vyvanse is now approved for both children and adults (20 mg, 30 mg, 40 mg, 50 mg, 60 mg, 70 mg).
- Unlike in the United States, 10-mg capsules are not available.
17. Bringing Amphetamine-Based Medications Abroad
For more information, see Taking Stimulants Abroad
Frölich, Banaschewski, Spanagel, Döpfner, Lehmkuhl (2012): Die medikamentöse Behandlung der Aufmerksamkeitsdefizit-Hyperaktivitätsstörung im Kindes- und Jugendalter mit Amfetaminpräparaten; Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie (2012), 40, pp. 287-300. https://doi.org/10.1024/1422-4917/a000185 ↥
Arnold: Journal of Attention Disorders Vol. 3(4):200-211 (2000) Methylphenidate vs. amphetamine: Comparative review, n = 174 ↥ ↥
Childress, Komolova, Sallee (2019): An update on the pharmacokinetic considerations in the treatment of ADHD with long-acting methylphenidate and amphetamine formulations. Expert Opin Drug Metab Toxicol. 2019 Nov;15(11):937-974. doi: 10.1080/17425255.2019.1675636. PMID: 31581854. REVIEW ↥ ↥ ↥
Heal DJ, Smith SL, Gosden J, Nutt DJ (2013): Amphetamine, past and present–a pharmacological and clinical perspective. J Psychopharmacol. 2013 Jun;27(6):479-96. doi: 10.1177/0269881113482532. PMID: 23539642; PMCID: PMC3666194. REVIEW ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥
Edel, Vollmoeller (2006): Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung bei Erwachsenen, Springer, Seite 57 ↥ ↥
Easton N, Steward C, Marshall F, Fone K, Marsden C (2007): Effects of amphetamine isomers, methylphenidate and atomoxetine on synaptosomal and synaptic vesicle accumulation and release of dopamine and noradrenaline in vitro in the rat brain. Neuropharmacology. 2007 Feb;52(2):405-14. doi: 10.1016/j.neuropharm.2006.07.035. PMID: 17020775. ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥
Heikkila RE, Orlansky H, Mytilineou C, Cohen G (1975): Amphetamine: evaluation of d- and l-isomers as releasing agents and uptake inhibitors for 3H-dopamine and 3H-norepinephrine in slices of rat neostriatum and cerebral cortex. J Pharmacol Exp Ther. 1975 Jul;194(1):47-56. PMID: 1151755. ↥
Stahl (2013): Stahl’s Essential Psychopharmacology, 4. Auflage, Chapter 12: Attention deficit hyperactivity disorder and its treatment, Seite 491 ↥ ↥ ↥ ↥
Castellanos, Tannock (2002): Neuroscience of attention-deficit/hyperactivity disorder: The search for endophenotypes; Article in Nature reviews Neuroscience 3(8):617-28 · September 2002; DOI: 10.1038/nrn896, Seite 621 ↥
Davis, Hernandez, Stock (2020): Adolescent Polypharmacy and Serotonin Syndrome. Clin Neuropharmacol. 2020 Jan/Feb;43(1):28-30. doi: 10.1097/WNF.0000000000000375. PMID: 31934921. ↥ ↥ ↥
Patel P, Marwaha R, Molla M (2025): Dextroamphetamine-Amphetamine. 2025 Apr 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 29939585. ↥ ↥ ↥ ↥
Hutson PH, Pennick M, Secker R (2014): Preclinical pharmacokinetics, pharmacology and toxicology of lisdexamfetamine: a novel d-amphetamine pro-drug. Neuropharmacology. 2014 Dec;87:41-50. doi: 10.1016/j.neuropharm.2014.02.014. PMID: 24594478. REVIEW ↥ ↥ ↥
Prox-Vagedes, Ohlmeier in Ohlmeier, Roy (Hrsg.) (2012): ADHS bei Erwachsenen – Ein Leben in Extremen, Kapitel 5: Die Suche nach dem Rausch: Substanzabhängigkeit bei ADHS, Seite 101, mwNw ↥
Kämmerer W (2024): Comparative pharmacology and abuse potential of oral dexamphetamine and lisdexamfetamine-A literature review. Hum Psychopharmacol. 2024 Jul 18:e2910. doi: 10.1002/hup.2910. PMID: 39024047. REVIEW ↥ ↥ ↥
Sharman J, Pennick M (2023): Lisdexamfetamine prodrug activation by peptidase-mediated hydrolysis in the cytosol of red blood cells. Neuropsychiatr Dis Treat. 2014 Nov 28;10:2275-80. doi: 10.2147/NDT.S70382. PMID: 25489246; PMCID: PMC4257105. ↥
Seymur, Shapiro (1958): Analeptic amides of d-a Methylphenethylamine, Journal of the AmericanChemical Society 1958, S. 6065-6071 ↥
https://www.adhspedia.de/wiki/Umrechnungstabelle_Medikamente ↥
Stutzman DL, Dopheide JA (2024): Practice Pearls for Stimulant Treatment of Attention-Deficit/Hyperactivity Disorder in Youth. J Pediatr Pharmacol Ther. 2024 Jun;29(3):215-231. doi: 10.5863/1551-6776-29.3.215. PMID: 38863854; PMCID: PMC11163912. ↥
Pharmazeutische Zeitung: Lisdexamfetamin|Elvanse®|71|2013 ↥ ↥
Childress, Komolova, Sallee (2019): An update on the pharmacokinetic considerations in the treatment of ADHD with long-acting methylphenidate and amphetamine formulations. Expert Opin Drug Metab Toxicol. 2019 Nov;15(11):937-974. doi: 10.1080/17425255.2019.1675636. PMID: 31581854. ↥ ↥ ↥ ↥ ↥ ↥ ↥
Medikamio.com: Elvanse Abruf 09.07.2023 ↥
Heal DJ, Gosden J, Smith SL (2024): Stimulant prodrugs: A pharmacological and clinical assessment of their role in treating ADHD and binge-eating disorder. Adv Pharmacol. 2024;99:251-286. doi: 10.1016/bs.apha.2023.10.002. PMID: 38467483. REVIEW ↥
Krishnan SM, Stark JG (2008): Multiple daily-dose pharmacokinetics of lisdexamfetamine dimesylate in healthy adult volunteers. Curr Med Res Opin. 2008 Jan;24(1):33-40. doi: 10.1185/030079908x242737. PMID: 18021493. ↥
Mohammadi M, Akhondzadeh S (2011): Advances and considerations in attention-deficit/hyperactivity disorder pharmacotherapy. Acta Med Iran. 2011;49(8):487-98. PMID: 22009816. REVIEW ↥
Stahl (2013): Stahl’s Essential Psychopharmacology, 4. Auflage, Chapter 12: Attention deficit hyperactivity disorder and its treatment, Seite 491 ↥
Huberman (2023): Adderall, Stimulants & Modafinil for ADHD: Short- & Long-Term Effects | Huberman Lab Podcast, english ↥
Buoli, Serati, Cahn (2016): Alternative pharmacological strategies for adult ADHD treatment: a systematic review. Expert Rev Neurother. 2016;16(2):131-44. doi: 10.1586/14737175.2016.1135735. PMID: 26693882. REVIEW ↥ ↥ ↥
Biel, Bopp (1978): Amphetamines: Structure-Activity Relationships, in: Iversen et al. (Hrsg.), Handbook of Psychopharmacology, Vol. 11: Stimulants, Boston 1978, S. 1-39, Tabelle 13 ↥
Paz-Ramos MI, Cruz SL, Violante-Soria V (2023): Amphetamine-type Stimulants: Novel Insights into their Actions and use Patterns. Rev Invest Clin. 2023;75(3):143-157. doi: 10.24875/RIC.23000110. PMID: 37441770. REVIEW ↥
so noch Edel, Vollmoeller (2006): Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung bei Erwachsenen, Springer, Seite 57 ↥
Takeda März 2024: Fachinformation Elvanse 20 mg/30 mg/40 mg/50 mg/60 mg/70 mg, unter 4.1. ↥
Döpfner, Universitätsklinikum Köln, https://www.adhs.info/fuer-erwachsene/therapie-und-andere-hilfen/, Ansicht 03.10.25 ↥
Lisdexamfetamin – jetzt auch für Erwachsene zugelassen – Kompendium psychiatrische Pharmakotherapie, Springer. ↥
Pharmazeutische Zeitung: Arzneistoffe: Lisdexamfetamin|Elvanse®|71|2013 ↥
Kölle, Mackert, Philipsen (2021): Pharmakotherapie der ADHS im Erwachsenenalter; Psychopharmakotherapie, Abruf 03.10.2025 ↥
Winkler (2024): Elvanse für Alle: Eine Neuerung in der ADHS-Behandlung, ADHSSpektrum.com, Abruf 03.10.2025 ↥
Ratiopharm (Juni 2024): Lisdexamfetamin-ratiopharm Erwachsene Hartkapseln, Version 5 ↥
Banaschewski T (Leitlinienkoordinator), Hohmann, Millenet et al (2018): Langfassung der interdisziplinären evidenz- und konsensbasierten (S3) Leitlinie „Aufmerksamkeitsdefizit- / Hyperaktivitätsstörung (ADHS) im Kindes-, Jugend- und Erwachsenenalter“ AWMF-Registernummer 028-045 ↥
Hohmann-Jeddi (2024) Was bei Erwachsenen anders ist; Interviewaussage Retz; Pharmazeutische Zeitung. Ansicht ß3.10.2025 ↥
Zusammenfassende Dokumentation über eine Änderung der Arzneimittel-Richtlinie (AM-RL): Anlage XII – Nutzenbewertung von Arzneimitteln mit neuen Wirkstoffen nach § 35a SGB V Lisdexamfetamindimesilat (17. Oktober 2019) - ohne Stellungnahme GBA ↥
Edel, Vollmoeller (2006): Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung bei Erwachsenen, Springer, Seite 57, Stand 2006 ↥ ↥
Fouladvand, Hankosky, Bush, Chen, Dwoskin, Freeman, Henderson, Kantak, Talbert, Tao, Zhang (2019): Predicting substance use disorder using long-term attention deficit hyperactivity disorder medication records in Truven. Health Informatics J. 2019 May 19:1460458219844075. doi: 10.1177/1460458219844075. ↥
Rösler, Retz (2020): Medikamentöse Therapie der ADHS bei Erwachsenen; Psychiatrie up2date 2020; 14: 59–75 ↥
Kooij, Bijlenga, Salerno, Jaeschke, Bitter, Balázs, Thome, Dom, Kasper, Filipe, Stes, Mohr, Leppämäki, Brugué, Bobes, Mccarthy, Richarte, Philipsen, Pehlivanidis, Niemela, Styr, Semerci, Bolea-Alamanac, Edvinsson, Baeyens, Wynchank, Sobanski, Philipsen, McNicholas, Caci, Mihailescu, Manor, Dobrescu, Krause, Fayyad, Ramos-Quiroga, Foeken, Rad, Adamou, Ohlmeier, Fitzgerald, Gill, Lensing, Mukaddes, Brudkiewicz, Gustafsson, Tania, Oswald, Carpentier, De Rossi, Delorme, Simoska, Pallanti, Young, Bejerot, Lehtonen, Kustow, Müller-Sedgwick, Hirvikoski, Pironti, Ginsberg, Félegeházy, Garcia-Portilla, Asherson (2018): Updated European Consensus Statement on diagnosis and treatment of adult ADHD, European Psychiatrie, European Psychiatry 56 (2019) 14–34, http://dx.doi.org/10.1016/j.eurpsy.2018.11.001, Seite 22, 7.4.1. ↥ ↥ ↥
Cortese, Adamo, Del Giovane, Mohr-Jensen, Hayes, Carucci, Atkinson, Tessari, Banaschewski, Coghill, Hollis, Simonoff, Zuddas, Barbui, Purgato, Steinhausen, Shokraneh, Xia, Cipriani (2018): Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis. Lancet Psychiatry. 2018 Sep;5(9):727-738. doi: 10.1016/S2215-0366(18)30269-4. ↥ ↥ ↥
Heal, Cheetham, Smith (2009): The neuropharmacology of ADHD drugs in vivo: insights on efficacy and safety. Neuropharmacology. 2009 Dec;57(7-8):608-18. doi: 10.1016/j.neuropharm.2009.08.020. ↥ ↥ ↥ ↥ ↥ ↥ ↥
Faraone (2018): The pharmacology of amphetamine and methylphenidate: Relevance to the neurobiology of attention-deficit/hyperactivity disorder and other psychiatric comorbidities. Neurosci Biobehav Rev. 2018 Apr;87:255-270. doi: 10.1016/j.neubiorev.2018.02.001. PMID: 29428394. ↥ ↥ ↥
Visentin R, Dalla Man C, Kovatchev B, Cobelli C (2014): The university of Virginia/Padova type 1 diabetes simulator matches the glucose traces of a clinical trial. Diabetes Technol Ther. 2014 Jul;16(7):428-34. doi: 10.1089/dia.2013.0377. PMID: 24571584; PMCID: PMC4074748. ↥
Gutiérrez-Casares JR, Quintero J, Segú-Vergés C, Rodríguez Monterde P, Pozo-Rubio T, Coma M, Montoto C (2023): In silico clinical trial evaluating lisdexamfetamine’s and methylphenidate’s mechanism of action computational models in an attention-deficit/hyperactivity disorder virtual patients’ population. Front Psychiatry. 2023 Jun 2;14:939650. doi: 10.3389/fpsyt.2023.939650. PMID: 37333910; PMCID: PMC10273406. ↥
Seeman P, Madras BK (1998): Anti-hyperactivity medication: methylphenidate and amphetamine. Mol Psychiatry. 1998 Sep;3(5):386-96. doi: 10.1038/sj.mp.4000421. PMID: 9774771. REVIEW ↥ ↥ ↥ ↥ ↥ ↥
Covey DP, Juliano SA, Garris PA (2013): Amphetamine elicits opposing actions on readily releasable and reserve pools for dopamine. PLoS One. 2013 May 3;8(5):e60763. doi: 10.1371/journal.pone.0060763. PMID: 23671560; PMCID: PMC3643976. ↥ ↥ ↥
Schmitz Y, Lee CJ, Schmauss C, Gonon F, Sulzer D (2001): Amphetamine distorts stimulation-dependent dopamine overflow: effects on D2 autoreceptors, transporters, and synaptic vesicle stores. J Neurosci. 2001 Aug 15;21(16):5916-24. doi: 10.1523/JNEUROSCI.21-16-05916.2001. PMID: 11487614; PMCID: PMC6763160. ↥ ↥
Sulzer D, Rayport S (1990): Amphetamine and other psychostimulants reduce pH gradients in midbrain dopaminergic neurons and chromaffin granules: a mechanism of action. Neuron. 1990 Dec;5(6):797-808. doi: 10.1016/0896-6273(90)90339-h. PMID: 2268433. ↥ ↥
Schmitz Y, Schmauss C, Sulzer D. Altered dopamine release and uptake kinetics in mice lacking D2 receptors. J Neurosci. 2002 Sep 15;22(18):8002-9. doi: 10.1523/JNEUROSCI.22-18-08002.2002. PMID: 12223553; PMCID: PMC6758092. ↥ ↥ ↥
Frölich, Banaschewski, Spanagel, Döpfner, Lehmkuhl (2012): Die medikamentöse Behandlung der Aufmerksamkeitsdefizit-Hyperaktivitätsstörung im Kindes- und Jugendalter mit Amphetaminpräparaten; Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie (2012), 40, pp. 287-300. https://doi.org/10.1024/1422-4917/a000185 ↥ ↥ ↥
Stahl (2013): Stahl’s Essential Psychopharmacology, 4. Auflage, Chapter 12: Attention deficit hyperactivity disorder and its treatment, Seite 490 ↥ ↥ ↥ ↥ ↥
Markowitz, Patrick (2001): Pharmacokinetic and pharmacodynamic drug interactions in the treatment of attention-deficit hyperactivity disorder. Clin Pharmacokinet. 2001;40(10):753-72. doi: 10.2165/00003088-200140100-00004. PMID: 11707061. REVIEW ↥
Steinhausen, Rothenberger, Döpfner (2010): Handbuch ADHS, Seite 84, 85 ↥ ↥ ↥
Hodgkins P, Shaw M, Coghill D, Hechtman L (2012): Amfetamine and methylphenidate medications for attention-deficit/hyperactivity disorder: complementary treatment options. Eur Child Adolesc Psychiatry. 2012 Sep;21(9):477-92. doi: 10.1007/s00787-012-0286-5. PMID: 22763750; PMCID: PMC3432777. REVIEW ↥ ↥ ↥
Castellanos, Tannock (2002): Neuroscience of attention-deficit/hyperactivity disorder: The search for endophenotypes; Article in Nature reviews Neuroscience 3(8):617-28 · September 2002; DOI: 10.1038/nrn896, Seite 621, mwNw ↥ ↥
Khoshbouei H, Sen N, Guptaroy B, Johnson L’, Lund D, Gnegy ME, Galli A, Javitch JA (2004): N-terminal phosphorylation of the dopamine transporter is required for amphetamine-induced efflux. PLoS Biol. 2004 Mar;2(3):E78. doi: 10.1371/journal.pbio.0020078. PMID: 15024426; PMCID: PMC368172. ↥ ↥ ↥
Daniels GM, Amara SG (1999):. Regulated trafficking of the human dopamine transporter. Clathrin-mediated internalization and lysosomal degradation in response to phorbol esters. J Biol Chem. 1999 Dec 10;274(50):35794-801. doi: 10.1074/jbc.274.50.35794. PMID: 10585462. ↥
Granas C, Ferrer J, Loland CJ, Javitch JA, Gether U (2003): N-terminal truncation of the dopamine transporter abolishes phorbol ester- and substance P receptor-stimulated phosphorylation without impairing transporter internalization. J Biol Chem. 2003 Feb 14;278(7):4990-5000. doi: 10.1074/jbc.M205058200. PMID: 12464618. ↥
Giambalvo CT (2003): Differential effects of amphetamine transport vs. dopamine reverse transport on particulate PKC activity in striatal synaptoneurosomes. Synapse. 2003 Aug;49(2):125-33. doi: 10.1002/syn.10223. PMID: 12740868. ↥
Foster JD, Pananusorn B, Vaughan RA (2002): Dopamine transporters are phosphorylated on N-terminal serines in rat striatum. J Biol Chem. 2002 Jul 12;277(28):25178-86. doi: 10.1074/jbc.M200294200. PMID: 11994276. ↥
Saunders C, Ferrer JV, Shi L, Chen J, Merrill G, Lamb ME, Leeb-Lundberg LM, Carvelli L, Javitch JA, Galli A (2000): Amphetamine-induced loss of human dopamine transporter activity: an internalization-dependent and cocaine-sensitive mechanism. Proc Natl Acad Sci U S A. 2000 Jun 6;97(12):6850-5. doi: 10.1073/pnas.110035297. PMID: 10823899; PMCID: PMC18764. ↥ ↥
Mulvihill (2019): Presynaptic regulation of dopamine release: Role of the DAT and VMAT2 transporters. Neurochem Int. 2019 Jan;122:94-105. doi: 10.1016/j.neuint.2018.11.004. PMID: 30465801. ↥
Robertson SD, Matthies HJ, Galli A (2009): A closer look at amphetamine-induced reverse transport and trafficking of the dopamine and norepinephrine transporters. Mol Neurobiol. 2009 Apr;39(2):73-80. doi: 10.1007/s12035-009-8053-4. PMID: 19199083; PMCID: PMC2729543. REVIEW ↥
Freyberg Z, Sonders MS, Aguilar JI, Hiranita T, Karam CS, Flores J, Pizzo AB, Zhang Y, Farino ZJ, Chen A, Martin CA, Kopajtic TA, Fei H, Hu G, Lin YY, Mosharov EV, McCabe BD, Freyberg R, Wimalasena K, Hsin LW, Sames D, Krantz DE, Katz JL, Sulzer D, Javitch JA (2016): Mechanisms of amphetamine action illuminated through optical monitoring of dopamine synaptic vesicles in Drosophila brain. Nat Commun. 2016 Feb 16;7:10652. doi: 10.1038/ncomms10652. PMID: 26879809; PMCID: PMC4757768. ↥
Edinoff, Akuly, Wagner, Boudreaux, Kaplan, Yusuf, Neuchat, Cornett, Boyer, Kaye, Kaye (2021): Viloxazine in the Treatment of Attention Deficit Hyperactivity Disorder. Front Psychiatry. 2021 Dec 17;12:789982. doi: 10.3389/fpsyt.2021.789982. PMID: 34975586; PMCID: PMC8718796., REVIEW ↥ ↥
Daberkow DP, Brown HD, Bunner KD, Kraniotis SA, Doellman MA, Ragozzino ME, Garris PA, Roitman MF (2013): Amphetamine paradoxically augments exocytotic dopamine release and phasic dopamine signals. J Neurosci. 2013 Jan 9;33(2):452-63. doi: 10.1523/JNEUROSCI.2136-12.2013. PMID: 23303926; PMCID: PMC3711765. ↥
Mergy MA, Gowrishankar R, Davis GL, Jessen TN, Wright J, Stanwood GD, Hahn MK, Blakely RD (2014): Genetic targeting of the amphetamine and methylphenidate-sensitive dopamine transporter: on the path to an animal model of attention-deficit hyperactivity disorder. Neurochem Int. 2014 Jul;73:56-70. doi: 10.1016/j.neuint.2013.11.009. PMID: 24332984; PMCID: PMC4177817. ↥
Revel FG, Moreau JL, Gainetdinov RR, Ferragud A, Velázquez-Sánchez C, Sotnikova TD, Morairty SR, Harmeier A, Groebke Zbinden K, Norcross RD, Bradaia A, Kilduff TS, Biemans B, Pouzet B, Caron MG, Canales JJ, Wallace TL, Wettstein JG, Hoener MC (2012): Trace amine-associated receptor 1 partial agonism reveals novel paradigm for neuropsychiatric therapeutics. Biol Psychiatry. 2012 Dec 1;72(11):934-42. doi: 10.1016/j.biopsych.2012.05.014. PMID: 22705041. ↥
Di Cara B, Maggio R, Aloisi G, Rivet JM, Lundius EG, Yoshitake T, Svenningsson P, Brocco M, Gobert A, De Groote L, Cistarelli L, Veiga S, De Montrion C, Rodriguez M, Galizzi JP, Lockhart BP, Cogé F, Boutin JA, Vayer P, Verdouw PM, Groenink L, Millan MJ (2011): Genetic deletion of trace amine 1 receptors reveals their role in auto-inhibiting the actions of ecstasy (MDMA). J Neurosci. 2011 Nov 23;31(47):16928-40. doi: 10.1523/JNEUROSCI.2502-11.2011. PMID: 22114263; PMCID: PMC6623861. ↥
Sitte HH, Freissmuth M (2015): Amphetamines, new psychoactive drugs and the monoamine transporter cycle. Trends Pharmacol Sci. 2015 Jan;36(1):41-50. doi: 10.1016/j.tips.2014.11.006. PMID: 25542076; PMCID: PMC4502921. REVIEW ↥
Mulvihill (2019): Presynaptic regulation of dopamine release: Role of the DAT and VMAT2 transporters. Neurochem Int. 2019 Jan;122:94-105. doi: 10.1016/j.neuint.2018.11.004. PMID: 30465801. REVIEW ↥
Quansah, Ruiz-Rodado, Grootveld, Zetterström (2018): Methylphenidate alters monoaminergic and metabolic pathways in the cerebellum of adolescent rats. Eur Neuropsychopharmacol. 2018 Feb 22. pii: S0924-977X(18)30043-9. doi: 10.1016/j.euroneuro.2018.02.002. ↥
Quansah, Zetterström (2019): Chronic methylphenidate preferentially alters catecholamine protein targets in the parietal cortex and ventral striatum. Neurochem Int. 2019 Jan 17;124:193-199. doi: 10.1016/j.neuint.2019.01.016. ↥
Felmer AC, Janson MT, Summers KE, Wallace LJ (2019):. Extracellular dopamine kinetic parameters consistent with amphetamine effects. Synapse. 2019 Dec;73(12):e22129. doi: 10.1002/syn.22129. PMID: 31449701. ↥
Jones SR, Gainetdinov RR, Wightman RM, Caron MG (1998): Mechanisms of amphetamine action revealed in mice lacking the dopamine transporter. J Neurosci. 1998 Mar 15;18(6):1979-86. doi: 10.1523/JNEUROSCI.18-06-01979.1998. PMID: 9482784; PMCID: PMC6792915. ↥
Müller, Candrian, Kropotov (2011), ADHS – Neurodiagnostik in der Praxis, Springer, Seiten 21, 86 ↥ ↥
Ruskin DN, Bergstrom DA, Shenker A, Freeman LE, Baek D, Walters JR (2001): Drugs used in the treatment of attention-deficit/hyperactivity disorder affect postsynaptic firing rate and oscillation without preferential dopamine autoreceptor action. Biol Psychiatry. 2001 Feb 15;49(4):340-50. doi: 10.1016/s0006-3223(00)00987-2. PMID: 11239905. ↥ ↥
Seeman P, Madras BK (1998): Anti-hyperactivity medication: methylphenidate and amphetamine. Mol Psychiatry. 1998 Sep;3(5):386-96. doi: 10.1038/sj.mp.4000421. PMID: 9774771. REVIEW ↥ ↥ ↥ ↥
Janenaite, Vengeliene, Bespalov, Behl (2017): Potential role of tyrosine hydroxylase in the loss of psychostimulant effect of amphetamine under conditions of impaired dopamine transporter activity. Behav Brain Res. 2017 Sep 15;334:105-108. doi: 10.1016/j.bbr.2017.07.028. PMID: 28750831. ↥
Rebec GV, Zimmerman KS (1980): Opposite effects of D-amphetamine on spontaneous neuronal activity in the neostriatum and nucleus accumbens. Brain Res. 1980 Nov 17;201(2):485-91. doi: 10.1016/0006-8993(80)91058-6. PMID: 7191347. ↥ ↥ ↥ ↥
Hansen EL, McKenzie GM (1979): Dexamphetamine increases striatal neuronal firing in freely moving rats. Neuropharmacology. 1979 Jun;18(6):547-52. doi: 10.1016/0028-3908(79)90099-6. PMID: 573376. ↥
Shi WX, Pun CL, Zhang XX, Jones MD, Bunney BS (2000): Dual effects of D-amphetamine on dopamine neurons mediated by dopamine and nondopamine receptors. J Neurosci. 2000 May 1;20(9):3504-11. doi: 10.1523/JNEUROSCI.20-09-03504.2000. PMID: 10777813; PMCID: PMC6773133. ↥ ↥
Newcorn JH, Ivanov I, Krone B, Li X, Duhoux S, White S, Schulz KP, Bédard AV, Pedraza J, Adler L, Blair RJ (2023): Neurobiological basis of reinforcement-based decision making in adults with ADHD treated with lisdexamfetamine dimesylate: Preliminary findings and implications for mechanisms influencing clinical improvement. J Psychiatr Res. 2023 Dec 3;170:19-26. doi: 10.1016/j.jpsychires.2023.11.037. PMID: 38101205. ↥
Schiffer WK, Volkow ND, Fowler JS, Alexoff DL, Logan J, Dewey SL (2006): Therapeutic doses of amphetamine or methylphenidate differentially increase synaptic and extracellular dopamine. Synapse. 2006 Mar 15;59(4):243-51. doi: 10.1002/syn.20235. PMID: 16385551. ↥ ↥
Marinelli M, McCutcheon JE (2014): Heterogeneity of dopamine neuron activity across traits and states. Neuroscience. 2014 Dec 12;282:176-97. doi: 10.1016/j.neuroscience.2014.07.034. PMID: 25084048; PMCID: PMC4312268. REVIEW ↥
Paladini CA, Fiorillo CD, Morikawa H, Williams JT (2001): Amphetamine selectively blocks inhibitory glutamate transmission in dopamine neurons. Nat Neurosci. 2001 Mar;4(3):275-81. doi: 10.1038/85124. PMID: 11224544. ↥
Howlett DR, Nahorski SR (1979): Acute and chronic amphetamine treatments modulate striatal dopamine receptor binding sites. Brain Res. 1979 Jan 26;161(1):173-8. doi: 10.1016/0006-8993(79)90206-3. PMID: 758968. ↥ ↥
Mang (2018): 05. Monoamine 2: Amphetamin, Ritalin (ADHS), Cocain, Tricyclika, Videovorlesung. ca. bei Minute 14:50. ↥ ↥
Kuczenski R, Segal DS (1997): Effects of methylphenidate on extracellular dopamine, serotonin, and norepinephrine: comparison with amphetamine. J Neurochem. 1997 May;68(5):2032-7. doi: 10.1046/j.1471-4159.1997.68052032.x. Erratum in: J Neurochem 1997 Sep;69(3):1332. PMID: 9109529. ↥ ↥
Lahey (Hrsg.) (2012): Advances in Clinical Child Psychology, Band 9, S. 187, mit Verweis auf [Brown, Ebert, Hunt, Rapoport (1981): Urinary 3-methoxy-4-hydroxyphenylglycol and homovanillic acid response to d-amphetamine in hyperactive children; Biological Psychiatry, Vol 16(8), Aug 1981, 779-787 ↥
Shekim, Dekirmenjian, Chapel, (1979): Urinary MHPG excretion in minimal brain dysfunction and its modification by d-amphetamine; The American Journal of Psychiatry, Vol 136(5), May 1979, 667-671. http://dx.doi.org/10.1176/ajp.136.5.667 ↥
Shen, Wang (1984): Urinary 3-methoxy-4-hydroxyphenylglycol sulfate excretion in seventy-three schoolchildren with minimal brain dysfunction syndrome.Biological Psychiatry [1984, 19(6):861-870]; PMID:6743722 ↥
Lahey (Hrsg.) (2012): Advances in Clinical Child Psychology, Band 9, S. 187, mit Verweis u.a. auf Shekim, Dekirmenjian, Chapel, (1979): Urinary MHPG excretion in minimal brain dysfunction and its modification by d-amphetamine; The American Journal of Psychiatry, Vol 136(5), May 1979, 667-671. http://dx.doi.org/10.1176/ajp.136.5.667 ↥
Paladini CA, Williams JT (2004): Noradrenergic inhibition of midbrain dopamine neurons. J Neurosci. 2004 May 12;24(19):4568-75. doi: 10.1523/JNEUROSCI.5735-03.2004. PMID: 15140928; PMCID: PMC6729397. ↥
Shi WX, Zhang XY, Pun CL, Bunney BS (2007): Clozapine blocks D-amphetamine-induced excitation of dopamine neurons in the ventral tegmental area. Neuropsychopharmacology. 2007 Sep;32(9):1922-8. doi: 10.1038/sj.npp.1301334. PMID: 17299514. ↥
Shen, Shi (2020): Amphetamine promotes cortical Up state: Role of adrenergic receptors. Addict Biol. 2020 Jan 31;e12879. doi: 10.1111/adb.12879. PMID: 32003119. ↥
Shen, Shi (2021): Amphetamine Promotes Cortical Up State in Part Via Dopamine Receptors. Front Pharmacol. 2021 Aug 19;12:728729. doi: 10.3389/fphar.2021.728729. PMID: 34489713; PMCID: PMC8417369. ↥ ↥
Mang (2018): 05. Monoamine 2: Amphetamin, Ritalin (ADHS), Cocain, Tricyclika, Videovorlesung. ca. bei Minute 14:30. ↥ ↥ ↥
Heal DJ, Smith SL, Kulkarni RS, Rowley HL (2008): New perspectives from microdialysis studies in freely-moving, spontaneously hypertensive rats on the pharmacology of drugs for the treatment of ADHD. Pharmacol Biochem Behav. 2008 Aug;90(2):184-97. doi: 10.1016/j.pbb.2008.03.016. PMID: 18456311. ↥ ↥
Castellanos FX, Acosta MT (2011): Hacia un entendimiento de los mecanismos moleculares de los tratamientos farmacologicos del trastorno por deficit de atencion/hiperactividad [Towards an understanding of the molecular mechanisms underlying the pharmacological treatments of attention deficit hyperactivity disorder]. Rev Neurol. 2011 Mar 1;52 Suppl 1:S155-60. Spanish. PMID: 21365598. REVIEW ↥
Heinz (2000, 2013): Das dopaminerge Verstärkungssystem – Funktion, Interaktion mit anderen Neurotransmittersystemen und psychopathologische Korrelate, Seite 61 ↥
Callaway, Johnson, Gold, Nichols, Geyer (1991): Amphetamine derivatives induce locomotor hyperactivity by acting as indirect serotonin agonists; Psychopharmacology (Berl). 1991;104(3):293-301 ↥ ↥
Tsuchida, Kubo, Shintani, Abe, Köves, Uetsuki, Kuroda, Hashimoto, Baba (2009): Inhibitory effects of osemozotan, a serotonin 1A-receptor agonist, on methamphetamine-induced c-Fos expression in prefrontal cortical neurons. Biol Pharm Bull. 2009 Apr;32(4):728-31. doi: 10.1248/bpb.32.728. PMID: 19336914. ↥
Strajhar, Vizeli, Patt, Dolder, Kratschmar, Liechti, Odermatt (2018): Effects of lisdexamfetamine on plasma steroid concentrations compared with d-amphetamine in healthy subjects: A randomized, double-blind, placebo-controlled study. J Steroid Biochem Mol Biol. 2019 Feb;186:212-225. doi: 10.1016/j.jsbmb.2018.10.016. PMID: 30381248. ↥ ↥ ↥
Soto, Wilcox, Zhou, Kumar, Ator, Riddle, Wong, Weed (2013): Long-term exposure to oral methylphenidate or dl-amphetamine mixture in peri-adolescent rhesus monkeys: effects on physiology, behavior, and dopamine system development. Neuropsychopharmacology. 2012 Nov;37(12):2566-79. doi: 10.1038/npp.2012.119. Erratum in: Neuropsychopharmacology. 2013 May;38(6):1141. Kumar, Anil [added]. PMID: 22805599; PMCID: PMC3473325. ↥
Mattison, Plant, Lin, Chen, Chen, Twaddle, Doerge, Slikker, Patton, Hotchkiss, Callicott, Schrader, Turner, Kesner, Vitiello, Petibone, Morris (2011): Pubertal delay in male nonhuman primates (Macaca mulatta) treated with methylphenidate. Proc Natl Acad Sci U S A. 2011 Sep 27;108(39):16301-6. doi: 10.1073/pnas.1102187108. PMID: 21930929; PMCID: PMC3182701. ↥
Tsai, Chiao, Lu, Doong, Chen, Shih, Liaw, Wang, Wang (1996): Inhibition by amphetamine of testosterone secretion through a mechanism involving an increase of cyclic AMP production in rat testes. Br J Pharmacol. 1996 Jun;118(4):984-8. doi: 10.1111/j.1476-5381.1996.tb15496.x. PMID: 8799572; PMCID: PMC1909523. ↥ ↥
Tsai, Chen, Chiao, Lu, Lin, Yeh, Lo, Kau, Wang, Wang (1997): The role of cyclic AMP production, calcium channel activation and enzyme activities in the inhibition of testosterone secretion by amphetamine. Br J Pharmacol. 1997 Nov;122(5):949-55. doi: 10.1038/sj.bjp.0701463. PMID: 9384514; PMCID: PMC1565017. ↥
Angenoorth TJF, Stankovic S, Niello M, Holy M, Brandt SD, Sitte HH, Maier J (2021): Interaction Profiles of Central Nervous System Active Drugs at Human Organic Cation Transporters 1-3 and Human Plasma Membrane Monoamine Transporter. Int J Mol Sci. 2021 Nov 30;22(23):12995. doi: 10.3390/ijms222312995. PMID: 34884800; PMCID: PMC8657792. ↥ ↥
Amphoux A, Vialou V, Drescher E, Brüss M, Mannoury La Cour C, Rochat C, Millan MJ, Giros B, Bönisch H, Gautron S (2006): Differential pharmacological in vitro properties of organic cation transporters and regional distribution in rat brain. Neuropharmacology. 2006 Jun;50(8):941-52. doi: 10.1016/j.neuropharm.2006.01.005. PMID: 16581093. ↥ ↥ ↥
Orrico-Sanchez A, Chausset-Boissarie L, Alves de Sousa R, Coutens B, Rezai Amin S, Vialou V, Louis F, Hessani A, Dansette PM, Zornoza T, Gruszczynski C, Giros B, Guiard BP, Acher F, Pietrancosta N, Gautron S (2020): Antidepressant efficacy of a selective organic cation transporter blocker in a mouse model of depression. Mol Psychiatry. 2020 Jun;25(6):1245-1259. doi: 10.1038/s41380-019-0548-4. PMID: 31619760. ↥
Bacq A, Balasse L, Biala G, Guiard B, Gardier AM, Schinkel A, Louis F, Vialou V, Martres MP, Chevarin C, Hamon M, Giros B, Gautron S (2012): Organic cation transporter 2 controls brain norepinephrine and serotonin clearance and antidepressant response. Mol Psychiatry. 2012 Sep;17(9):926-39. doi: 10.1038/mp.2011.87. PMID: 21769100. ↥
Matochik, Liebenauer, King, Szymanski, Cohen, Zametkin (1994): Cerebral glucose metabolism in adults with attention defi cit hyperactivity disorder after chronic stimulant treatment. Am J Psychiatry 151: 658–664; Achtung, geringes N von 37; geringe Stichprobe mit n = 18; zitiert nach Edel, Vollmoeller (2006): Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung bei Erwachsenen, Springer, Seite 10 ↥
Stroemer, Kent, Hulsebosch (1998): Enhanced neocortical neural sprouting, synaptogenesis, and behavioral recovery with D-amphetamine therapy after neocortical infarction in rats; Stroke. 1998 Nov;29(11):2381-93; discussion 2393-5. ↥
Rau T, Ziemniak J, Poulsen D (2016): The neuroprotective potential of low-dose methamphetamine in preclinical models of stroke and traumatic brain injury. Prog Neuropsychopharmacol Biol Psychiatry. 2016 Jan 4;64:231-6. doi: 10.1016/j.pnpbp.2015.02.013. PMID: 25724762. REVIEW ↥
Jin C, Schachar R (2004): Methylphenidate treatment of attention-deficit/hyperactivity disorder secondary to traumatic brain injury: a critical appraisal of treatment studies. CNS Spectr. 2004 Mar;9(3):217-26. doi: 10.1017/s1092852900009019. PMID: 14999162. ↥
Takahashi, Ohmiya, Honda, Ni (2018): The KCNH3 inhibitor ASP2905 shows potential in the treatment of attention deficit/hyperactivity disorder. PLoS One. 2018 Nov 21;13(11):e0207750. doi: 10.1371/journal.pone.0207750. eCollection 2018. ↥
Hutson, Heins, Folgering (2015): Effects of lisdexamfetamine alone and in combination with s-citalopram on acetylcholine and histamine efflux in the rat pre-frontal cortex and ventral hippocampus. J Neurochem. 2015 Aug;134(4):693-703. doi: 10.1111/jnc.13157. ↥
Madras, Miller, Fischman (2005): The dopamine transporter and attention-deficit/hyperactivity disorder. Biol Psychiatry. 2005 Jun 1;57(11):1397-409. doi: 10.1016/j.biopsych.2004.10.011. PMID: 15950014. ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥
Nagy, Häge, Coghill, Caballero, Adey, Anderson, Sikirica, Cardo (2015): Functional outcomes from a head-to-head, randomized, double-blind trial of lisdexamfetamine dimesylate and atomoxetine in children and adolescents with attention-deficit/hyperactivity disorder and an inadequate response to methylphenidate.Eur Child Adolesc Psychiatry. 2016 Feb;25(2):141-9. doi: 10.1007/s00787-015-0718-0. ↥
Madhoo, Keefe, Roth, Sambunaris, Wu, Trivedi, Anderson, Lasser (2014): Lisdexamfetamine dimesylate augmentation in adults with persistent executive dysfunction after partial or full remission of major depressive disorder; Neuropsychopharmacology. 2014 May;39(6):1388-98. doi: 10.1038/npp.2013.334 n = 143 Erwachsene ↥
Coghill, Banaschewski, Nagy, Otero, Soutullo, Yan, Caballero, Zuddas (2017): Long-Term Safety and Efficacy of Lisdexamfetamine Dimesylate in Children and Adolescents with ADHD: A Phase IV, 2-Year, Open-Label Study in Europe.CNS Drugs. 2017 Jun 30. doi: 10.1007/s40263-017-0443-y; n = 314 ↥ ↥
Arnold: Journal of Attention Disorders Vol. 3(4):200-211 (2000) Methylphenidate vs. amphetamine: Comparative review n = 174 ↥
Müller, Candrian, Kropotov (2011), ADHS – Neurodiagnostik in der Praxis, Seite 21 ↥
Diamond: Attention-deficit disorder (attention-deficit/hyperactivity disorder without hyperactivity): A neurobiologically and behaviorally distinct disorder from attention-deficit (with hyperactivity), Development and Psychopathology 17 (2005), 807–825, Seite 811 ↥
Liddle, Hollis, Batty, Groom, Totman, Liotti, Scerif, Liddle (2011): Task-related default mode network modulation and inhibitory control in ADHD: effects of motivation and methylphenidate. J Child Psychol Psychiatry. 2011 Jul;52(7):761-71. doi: 10.1111/j.1469-7610.2010.02333.x. ↥
ADHS-Chaoten;Thread: Amphetamin und Methylphenidat für Depressionen ↥
Adler, Goodman, Weisler, Hamdani, Roth (2009): Effect of lisdexamfetamine dimesylate on sleep in adults with attention-deficit/hyperactivity disorder. Behav Brain Funct. 2009 Aug 3;5:34. doi: 10.1186/1744-9081-5-34. PMID: 19650932; PMCID: PMC2732626. ↥
Giblin, Strobel (2011): Effect of lisdexamfetamine dimesylate on sleep in children with ADHD. J Atten Disord. 2011 Aug;15(6):491-8. doi: 10.1177/1087054710371195. PMID: 20574056. ↥
López FA, Leroux JR (2013): Long-acting stimulants for treatment of attention-deficit/hyperactivity disorder: a focus on extended-release formulations and the prodrug lisdexamfetamine dimesylate to address continuing clinical challenges. Atten Defic Hyperact Disord. 2013 Sep;5(3):249-65. doi: 10.1007/s12402-013-0106-x. PMID: 23564273; PMCID: PMC3751218. REVIEW ↥
Castells X1, Ramos-Quiroga JA, Bosch R, Nogueira M, Casas (2011): Amphetamines for Attention Deficit Hyperactivity Disorder (ADHD) in adults; Cochrane Database Syst Rev. 2011 Jun 15;(6):CD007813. doi: 10.1002/14651858.CD007813.pub2. n = 1.071 ↥
Hogan (2023) National Health Service, Oxford Health Drugs &Therapeutics Group: Guidance for switching between lis-dexamfetamine and dexamfetamine ↥
Mattay, Goldberg, Fera, Hariri, Tessitore, Egan, Kolachana, Callicott, Weinberger (2003): Catechol O-methyltransferase val158-met genotype and individual variation in the brain response to amphetamine; doi: 10.1073/pnas.0931309100; PNAS May 13, 2003 vol. 100 no. 10 6186-6191 ↥
Farhat LC, Sugaya LS, Bloch MH, Childress A, Cortese S, Fatori D, Salum GA, Rohde LA, Polanczyk GV (2025): Moderators of Response to Stimulants for Preschool Attention-Deficit/Hyperactivity Disorder. J Am Acad Child Adolesc Psychiatry. 2025 Sep 18:S0890-8567(25)02051-9. doi: 10.1016/j.jaac.2025.09.012. PMID: 40975435. ↥
Gul MK, Cagir B, Demirci E, Ozmen S (2025): The relationship between response to treatment and perceived stress, childhood trauma and psychological resilience in anxiety disorders and attention-deficit hyperactivity disorder in adolescents: A comparative study from Türkiye. Arch Psychiatr Nurs. 2025 Apr;55:151856. doi: 10.1016/j.apnu.2025.151856. PMID: 40204375. ↥
Oswald, Wand, Kuwabara, Wong, Zhu, Brasic (2014): History of childhood adversity is positively associated with ventral striatal dopamine responses to amphetamine. Psychopharmacology (Berl). 2014 Jun;231(12):2417-33. doi: 10.1007/s00213-013-3407-z. PMID: 24448898; PMCID: PMC4040334. ↥
Childress, Newcorn, Cutler (2019): Gender Effects in the Efficacy of Racemic Amphetamine Sulfate in Children with Attention-Deficit/Hyperactivity Disorder. Adv Ther. 2019 Apr 10. doi: 10.1007/s12325-019-00942-5. ↥
Zhang Y, Li X, Liu Y, Li X, Liu D, Han Q, Liu X, Wang X, Li JD, Deng S (2025): Knockout of Bmal1 in dopaminergic neurons induces ADHD-like symptoms via hyperactive dopamine signaling in male mice. Behav Brain Funct. 2025 Jul 11;21(1):22. doi: 10.1186/s12993-025-00287-w. PMID: 40646562; PMCID: PMC12247330. ↥
Arnold (2000): L.E. Methylphenidate vs amphetamine: Comparative review, J. of Att. Disorders, 2000, Vol 3, 200ff, n = 174 ↥
Müller, Candrian, Kropotov (2011), ADHS – Neurodiagnostik in der Praxis, Springer, Seite 21 ↥
Castello et al. 1992, zitiert nach Arnold: Journal of Attention Disorders Vol. 3(4):200-211 (2000) Methylphenidate vs. amphetamine: Comparative review ↥ ↥
Brams, Weisler, Findling, Gasior, Hamdani, Ferreira-Cornwell, Squires: Maintenance of Efficacy of Lisdexamfetamine Dimesylate in Adults With Attention-Deficit/Hyperactivity Disorder: Randomized Withdrawal Design, J Clin Psychiatry 2012;73(7):977-983; 10.4088/JCP.11m07430 ↥
http://www.ads-hyperaktivitaet.de/FAQ/Infos/Medis/medis.html#1 ↥
Markowitz, Patrick (2017): The Clinical Pharmacokinetics of Amphetamines Utilized in the Treatment of Attention-Deficit/Hyperactivity Disorder. J Child Adolesc Psychopharmacol. 2017 Oct;27(8):678-689. doi: 10.1089/cap.2017.0071. PMID: 28910145. REVIEW ↥ ↥
Dolder, Strajhar, Vizeli, Hammann, Odermatt, Liechti (2017): Pharmacokinetics and Pharmacodynamics of Lisdexamfetamine Compared with D-Amphetamine in Healthy Subjects. Front Pharmacol. 2017 Sep 7;8:617. doi: 10.3389/fphar.2017.00617. PMID: 28936175; PMCID: PMC5594082. n = 24) Die Studie benennt allerdings nicht das Gewicht der Probanden, sodass keine Aussage über die Dosierung je kg Körpergewicht möglich ist. Das Gewicht ist jedoch bei der Amfetamindosierung ein relevanter Faktor.((Markowitz, Patrick (2017): The Clinical Pharmacokinetics of Amphetamines Utilized in the Treatment of Attention-Deficit/Hyperactivity Disorder. J Child Adolesc Psychopharmacol. 2017 Oct;27(8):678-689. doi: 10.1089/cap.2017.0071. PMID: 28910145. REVIEW ↥
Wang L, Kong Q, Li Y (2025): Real world pharmacovigilance comparison of viloxazine and dextroamphetamine adverse reaction profiles. Sci Rep. 2025 Aug 7;15(1):28919. doi: 10.1038/s41598-025-14385-2. PMID: 40775008; PMCID: PMC12332145. ↥
Amphetamines. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-2016 ↥
Ito, Onodera, Yamatodani, Watanabe, Sato (1997): The effect of methamphetamine on histamine release in the rat hypothalamus. Psychiatry Clin Neurosci. 1997 Apr;51(2):79-81. doi: 10.1111/j.1440-1819.1997.tb02911.x. PMID: 9141145. ↥
Ito, Onodera, Sakurai, Sato, Watanabe (1996): The effect of methamphetamine on histamine level and histidine decarboxylase activity in the rat brain. Brain Res. 1996 Sep 23;734(1-2):98-102. PMID: 8896814. ↥
Houghton, de Vries, Loss (2019): Psychostimulants/Atomoxetine and Serious Cardiovascular Events in Children with ADHD or Autism Spectrum Disorder. CNS Drugs. 2019 Nov 25. doi: 10.1007/s40263-019-00686-4. n = 2.566.995 ↥
Forns, Dudukina, Hägg, Szentkúti, Gembert, Plana, Gilsenan, Horváth-Puhó, Ehrenstein, Reutfors, Rebordosa )2022): Risk of Major Cardiovascular and Cerebrovascular Events in Users of Lisdexamfetamine and Other Medications for Attention-Deficit/Hyperactivity Disorder in Denmark and Sweden: A Population-Based Cohort Study. Neurol Ther. 2022 Aug 26. doi: 10.1007/s40120-022-00396-y. PMID: 36028603. n = 273.000 ↥
Harris E. Long-Term ADHD Medications and Cardiovascular Disease Risk. JAMA. 2023 Dec 26;330(24):2331. doi: 10.1001/jama.2023.24173. PMID: 38055293. n = 60.000 ↥
Chan M, Chan JJ, Wright JM (2025): Effect of amphetamines on blood pressure. Cochrane Database Syst Rev. 2025 Mar 28;3(3):CD007896. doi: 10.1002/14651858.CD007896.pub4. PMID: 40152309; PMCID: PMC11951410. REVIEW ↥
Manso, Morcillo, Pereira, Maldonado (2020): Tricotilomanía de nueva aparición durante el tratamiento con fármacos estimulantes. A propósito de dos casos clínicos pediátricos [New-onset trichotillomania during treatment with stimulant drugs. About two pediatric clinical cases]. Arch Argent Pediatr. 2020 Feb;118(1):e61-e62. Spanish. doi: 10.5546/aap.2020.e61. PMID: 31984712. ↥
Abdalla TE, Kotsonis D, Best J, Ramasamy R, Wood E (2021): Stimulant-Induced Pituitary Failure and Reversible Azoospermia. Cureus. 2021 Apr 3;13(4):e14269. doi: 10.7759/cureus.14269. PMID: 33959450; PMCID: PMC8093113. ↥
Assem-Hilger, Kasper (2005): Psychopharmaka und sexuelle Dysfunktion. Journa lfür Neurologie, Neurochirurgie und Psychiatrie; 2005, 30-36 ↥
Duca Y, Aversa A, Condorelli RA, Calogero AE, La Vignera S (2019): Substance Abuse and Male Hypogonadism. J Clin Med. 2019 May 22;8(5):732. doi: 10.3390/jcm8050732. PMID: 31121993; PMCID: PMC6571549. REVIEW ↥ ↥
Strajhar P, Vizeli P, Patt M, Dolder PC, Kratschmar DV, Liechti ME, Odermatt A (2019): Effects of lisdexamfetamine on plasma steroid concentrations compared with d-amphetamine in healthy subjects: A randomized, double-blind, placebo-controlled study. J Steroid Biochem Mol Biol. 2019 Feb;186:212-225. doi: 10.1016/j.jsbmb.2018.10.016. PMID: 30381248. n = 24 ↥
Yamamoto Y, Yamamoto K, Hayase T (1999): Effect of methamphetamine on male mice fertility. J Obstet Gynaecol Res. 1999 Oct;25(5):353-8. doi: 10.1111/j.1447-0756.1999.tb01176.x. PMID: 10533332. ↥
Lin JF, Lin YH, Liao PC, Lin YC, Tsai TF, Chou KY, Chen HE, Tsai SC, Hwang TI (2014): Induction of testicular damage by daily methamphetamine administration in rats. Chin J Physiol. 2014 Feb 28;57(1):19-30. doi: 10.4077/CJP.2014.BAB155. PMID: 24621335. ↥
Kaewman P, Nudmamud-Thanoi S, Thanoi S (2018): GABAergic Alterations in the Rat Testis after Methamphetamine Exposure. Int J Med Sci. 2018 Aug 10;15(12):1349-1354. doi: 10.7150/ijms.27609. PMID: 30275762; PMCID: PMC6158670. ↥
Dickerson SM, Walker DM, Reveron ME, Duvauchelle CL, Gore AC (2008): The recreational drug ecstasy disrupts the hypothalamic-pituitary-gonadal reproductive axis in adult male rats. Neuroendocrinology. 2008;88(2):95-102. doi: 10.1159/000119691. PMID: 18309234; PMCID: PMC2753463. ↥
Barenys M, Macia N, Camps L, de Lapuente J, Gomez-Catalan J, Gonzalez-Linares J, Borras M, Rodamilans M, Llobet JM (2009): Chronic exposure to MDMA (ecstasy) increases DNA damage in sperm and alters testes histopathology in male rats. Toxicol Lett. 2009 Dec 1;191(1):40-6. doi: 10.1016/j.toxlet.2009.08.002. PMID: 19683041. ↥ ↥
Yamamoto Y, Yamamoto K, Hayase T, Abiru H, Shiota K, Mori C (2002): Methamphetamine induces apoptosis in seminiferous tubules in male mice testis. Toxicol Appl Pharmacol. 2002 Feb 1;178(3):155-60. doi: 10.1006/taap.2001.9330. PMID: 11858731. ↥
Alavi SH, Taghavi MM, Moallem SA (2008): Evaluation of effects of methamphetamine repeated dosing on proliferation and apoptosis of rat germ cells. Syst Biol Reprod Med. 2008 Mar-Apr;54(2):85-91. doi: 10.1080/19396360801952078. PMID: 18446649. ↥
Nudmamud-Thanoi S, Thanoi S (2011): Methamphetamine induces abnormal sperm morphology, low sperm concentration and apoptosis in the testis of male rats. Andrologia. 2011 Aug;43(4):278-82. doi: 10.1111/j.1439-0272.2010.01071.x. PMID: 21486410. ↥
Saberi A, Sepehri G, Safi Z, Razavi B, Jahandari F, Divsalar K, Salarkia E (2017): Effects of Methamphetamine on Testes Histopathology and Spermatogenesis Indices of Adult Male Rats. Addict Health. 2017 Fall;9(4):199-205. PMID: 30574282; PMCID: PMC6294480. ↥
Mobaraki F, Seghatoleslam M, Fazel A, Ebrahimzadeh-Bideskan A (2018): Effects of MDMA (ecstasy) on apoptosis and heat shock protein (HSP70) expression in adult rat testis. Toxicol Mech Methods. 2018 Mar;28(3):219-229. doi: 10.1080/15376516.2017.1388461. PMID: 29105552. ↥
Levine LA, Betcher HK, Ziegelmann MJ, Bajic P (2020): Amphetamine/Dextroamphetamine Salts for Delayed Orgasm and Anorgasmia in Men: A Pilot Study. Urology. 2020 Aug;142:141-145. doi: 10.1016/j.urology.2020.04.081. PMID: 32360625. n = 17 ↥
Bartlik BD, Kaplan P, Kaplan HS (1995): Psychostimulants apparently reverse sexual dysfunction secondary to selective serotonin re-uptake inhibitors. J Sex Marital Ther. 1995 Winter;21(4):264-71. doi: 10.1080/00926239508414646. PMID: 8789508. ↥
Coskun M, Zoroglu S (2009): A report of two cases of sexual side effects with OROS methylphenidate. J Child Adolesc Psychopharmacol. 2009 Aug;19(4):477-9. doi: 10.1089/cap.2008.0161. PMID: 19702503. ↥
Cakin-Memik N, Yildiz O, Sişmanlar SG, Karakaya I, Ağaoğlu B (2010): Priapism associated with methylphenidate: a case report. Turk J Pediatr. 2010 Jul-Aug;52(4):430-4. PMID: 21043394. ↥
Ostdiek-Wille GP, Bavitz KC, Kohn TP, Deibert CM (2023): Attention-deficit hyperactivity disorder medication use is associated with testosterone hypofunction-results from a national claims database analysis. Int J Impot Res. 2023 Dec 21. doi: 10.1038/s41443-023-00805-2. PMID: 38129694. n = 34.448 ↥
Ermer J, Haffey MB, Richards C, Lasseter K, Adeyi B, Corcoran M, Stanton B, Martin P (2013): Double-blind, placebo-controlled, two-period, crossover trial to examine the pharmacokinetics of lisdexamfetamine dimesylate in healthy older adults. Neuropsychiatr Dis Treat. 2013;9:219-29. doi: 10.2147/NDT.S38377. PMID: 23431065; PMCID: PMC3575217. ↥
Mang (2018): 05. Monoamine 2: Amphetamin, Ritalin (ADHS), Cocain, Tricyclika, Videovorlesung. ca. bei Minute 38. ↥
Spiller HA, Hays HL, Aleguas A Jr (2013): Overdose of drugs for attention-deficit hyperactivity disorder: clinical presentation, mechanisms of toxicity, and management. CNS Drugs. 2013 Jul;27(7):531-43. doi: 10.1007/s40263-013-0084-8. PMID: 23757186. REVIEW ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥
Fitzgerald KT, Bronstein AC (2013): Adderall® (amphetamine-dextroamphetamine) toxicity. Top Companion Anim Med. 2013 Feb;28(1):2-7. doi: 10.1053/j.tcam.2013.03.002. PMID: 23796480. ↥ ↥ ↥ ↥ ↥ ↥ ↥
Honório da Silva JV, Erthal RP, Vercellone IC, Santos DPD, Ferraz CR, de Matos RLN, Gonçalves LED, Bracarense APFRL, Verri WA Jr, Câmara NOS, de Andrade FG, Fernandes GSA (2024): Lisdexamfetamine dimesylate-exposition in male rats during the peripubertal period impairs inflammatory mechanisms, antioxidant activity, and apoptosis process in kidneys of male pubertal rats. J Biochem Mol Toxicol. 2024 Aug;38(8):e23781. doi: 10.1002/jbt.23781. PMID: 39051179. ↥
Sharman J, Pennick M (2014): Lisdexamfetamine prodrug activation by peptidase-mediated hydrolysis in the cytosol of red blood cells. Neuropsychiatr Dis Treat. 2014 Nov 28;10:2275-80. doi: 10.2147/NDT.S70382. PMID: 25489246; PMCID: PMC4257105. ↥
Ward K, Citrome L (2018): Lisdexamfetamine: chemistry, pharmacodynamics, pharmacokinetics, and clinical efficacy, safety, and tolerability in the treatment of binge eating disorder. Expert Opin Drug Metab Toxicol. 2018 Feb;14(2):229-238. doi: 10.1080/17425255.2018.1420163. PMID: 29258368. REVIEW ↥ ↥ ↥
Glennon RA (2013): “Phenylisopropylamine stimulants: amphetamine-related agents”. In Lemke TL, Williams DA, Roche VF, Zito W (eds.). Foye’s principles of medicinal chemistry (7th ed.). Philadelphia, US: Wolters Kluwer Health/Lippincott Williams & Wilkins. pp. 646–648. ISBN 9781609133450 ↥
Glennon RA (2013): “Phenylisopropylamine stimulants: amphetamine-related agents”, Chapter 19 Hallucinogens, Stimulants, and Related Drugs of Abuse and Their Therapeutic Potential“. In Lemke TL, Williams DA, Roche VF, Zito W (eds.). Foye’s principles of medicinal chemistry (7th ed.). Philadelphia, US: Wolters Kluwer Health/Lippincott Williams & Wilkins. pp. 646–648. ISBN 9781609133450 ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥
ASATOOR AM, GALMAN BR, JOHNSON JR, MILNE MD (1965): THE EXCRETION OF DEXAMPHETAMINE AND ITS DERIVATIVES. Br J Pharmacol Chemother. 1965 Feb;24(1):293-300. doi: 10.1111/j.1476-5381.1965.tb02105.x. PMID: 14302363; PMCID: PMC1704066. ↥ ↥
Petri (2019): Analyse von CYP450-Wechselwirkungen: kleiner Aufwand, große Wirkung. Das Interaktionspotenzial der Stimulanzien und Nichtstimulanzien. Psychopharmakotherapie 2019;26:57–61. ↥
Stein MA, McGough JJ (2008): The pharmacogenomic era: promise for personalizing attention deficit hyperactivity disorder therapy. Child Adolesc Psychiatr Clin N Am. 2008 Apr;17(2):475-90, xi-xii. doi: 10.1016/j.chc.2007.11.009. PMID: 18295157; PMCID: PMC2413066. ↥
Gerlach S, Maruf AA, Shaheen SM, McCloud R, Heintz M, McAusland L, Arnold PD, Bousman CA (2024): Effect of CYP2D6 genetic variation on patient-reported symptom improvement and side effects among children and adolescents treated with amphetamines. Pharmacogenet Genomics. 2024 Jul 1;34(5):149-153. doi: 10.1097/FPC.0000000000000529. PMID: 38517706. n = 214 ↥
Patel JN, Morris SA, Torres R, Rhead B, Vlangos C, Mueller DJ, Brown LC, Lefkofsky H, Ali M, De La Vega FM, Barnes KC, Zoghbi A, Stanton JD, Badgeley MA (2024): Pharmacogenomic insights in psychiatric care: uncovering novel actionability, allele-specific CYP2D6 copy number variation, and phenoconversion in 15,000 patients. Mol Psychiatry. 2024 Nov;29(11):3495-3502. doi: 10.1038/s41380-024-02588-4. PMID: 38783055; PMCID: PMC11541190. n = 15.000 ↥
Helland A, Muller S, Spigset O, Krabseth HM, Hansen M, Skråstad RB (2025): Drug detection in oral fluid and urine after single therapeutic doses of dexamphetamine, lisdexamphetamine, and methylphenidate in healthy volunteers. J Anal Toxicol. 2025 Feb 15;49(2):65-72. doi: 10.1093/jat/bkae097. Erratum in: J Anal Toxicol. 2025 Mar 10;49(3):e1. doi: 10.1093/jat/bkaf008. PMID: 39697138; PMCID: PMC12217515. n = 22 ↥
Brown JT (2022): The Pharmacogenetic Impact on the Pharmacokinetics of ADHD Medications. Methods Mol Biol. 2022;2547:427-436. doi: 10.1007/978-1-0716-2573-6_15. PMID: 36068472. ↥
FDA: Table of Pharmacogenetic Associations, Pharmacogenetic Associations for which the Data Support Therapeutic Management Recommendations ↥
Stahl S M (2024): Stahl’s Essential Psychopharmacology Prescriber’s Guide 8. Edition ↥
Feder, J., Tien, E., & Puzantian, T. (2023). Child medication fact book for psychiatric practice. Carlat Publishing, LLC. ↥
Van Vyve L, Dierckx B, Lim CG, Danckaerts M, Koch BCP, Häge A, Banaschewski T (2024): Pharmacotherapy for ADHD in children and adolescents: A summary and overview of different European guidelines. Eur J Pediatr. 2024 Mar;183(3):1047-1056. doi: 10.1007/s00431-023-05370-w. PMID: 38095716. REVIEW ↥
Teva Pharmaceuticals USA, Inc. (2024): ADDERALL- dextroamphetamine saccharate, amphetamine aspartate,dextroamphetamine sulfate, and amphetamine sulfate tablet ↥
Schoretsanitis, de Leon, Eap, Kane, Paulzen (2019): Clinically Significant Drug-Drug Interactions with Agents for Attention-Deficit/Hyperactivity Disorder. CNS Drugs. 2019 Dec;33(12):1201-1222. doi: 10.1007/s40263-019-00683-7. ↥ ↥ ↥ ↥
Gelbe Liste CYP2D6, Abruf 12.02.23 ↥
Elbe, Black, McGrane, Procyshyn (2019): Clinical Handbook of Psychotropic Drugs für Children and Adolescents, 4. Auflage, S. 39 ↥
Haedener M, Weinmann W, Eich D, Liebrenz M, Wuethrich T, Buadze A (2021): Evaluating the reliability of hair analysis in monitoring the compliance of ADHD patients under treatment with Lisdexamphetamine. PLoS One. 2021 Mar 30;16(3):e0248747. doi: 10.1371/journal.pone.0248747. PMID: 33784320; PMCID: PMC8009440. ↥
Silva-Carvalho M, Barbosa DJ, Dias da Silva D, Dinis-Oliveira RJ (2025): Multidimensional Evaluation of Lisdexamfetamine: Pharmacology, Therapeutic Use, Toxicity and Forensic Implications. Basic Clin Pharmacol Toxicol. 2025 Nov;137(5):e70111. doi: 10.1111/bcpt.70111. PMID: 41001763; PMCID: PMC12464896. REVIEW ↥
Grady SE, Sarma SJ (2023): High-dose stimulants for adult ADHD. Current Psychiatry, 2023 ↥
Vo K, Neafsey PJ, Lin CA (2015): Concurrent use of amphetamine stimulants and antidepressants by undergraduate students. Patient Prefer Adherence. 2015 Jan 22;9:161-72. doi: 10.2147/PPA.S74602. PMID: 25653508; PMCID: PMC4309786. ↥ ↥
Law R, Lewis D, Hain D, Daut R, DelBello MP, Frazier JA, Newcorn JH, Nurmi E, Cogan ES, Wagner S, Johnson H, Lanchbury J (2022): Characterisation of seven medications approved for attention-deficit/hyperactivity disorder using in vitro models of hepatic metabolism. Xenobiotica. 2022 Nov 1:1-32. doi: 10.1080/00498254.2022.2141151. PMID: 36317558. ↥
Bach MV, Coutts RT, Baker GB (1999): Involvement of CYP2D6 in the in vitro metabolism of amphetamine, two N-alkylamphetamines and their 4-methoxylated derivatives. Xenobiotica. 1999 Jul;29(7):719-32. doi: 10.1080/004982599238344. PMID: 10456690. ↥ ↥
Wu D, Otton SV, Inaba T, Kalow W, Sellers EM (1997): Interactions of amphetamine analogs with human liver CYP2D6. Biochem Pharmacol. 1997 Jun 1;53(11):1605-12. doi: 10.1016/s0006-2952(97)00014-2. PMID: 9264312. ↥ ↥
de la Torre R, Yubero-Lahoz S, Pardo-Lozano R, Farré M (2012): MDMA, methamphetamine, and CYP2D6 pharmacogenetics: what is clinically relevant? Front Genet. 2012 Nov 12;3:235. doi: 10.3389/fgene.2012.00235. PMID: 23162568; PMCID: PMC3495276. ↥
Bach MV, Coutts RT, Baker GB (2000): Metabolism of N,N-dialkylated amphetamines, including deprenyl, by CYP2D6 expressed in a human cell line. Xenobiotica. 2000 Mar;30(3):297-306. doi: 10.1080/004982500237686. PMID: 10752644. ↥
Yamada H, Shiiyama S, Soejima-Ohkuma T, Honda S, Kumagai Y, Cho AK, Oguri K, Yoshimura H (1997): Deamination of amphetamines by cytochromes P450: studies on substrate specificity and regioselectivity with microsomes and purified CYP2C subfamily isozymes. J Toxicol Sci. 1997 Feb;22(1):65-73. doi: 10.2131/jts.22.65. PMID: 9076658. ↥
Tomkins DM, Otton SV, Joharchi N, Berns T, Wu D, Corrigall WA, Sellers EM (1997): Effect of CYP2D1 inhibition on the behavioural effects of d-amphetamine. Behav Pharmacol. 1997 Jun;8(2-3):223-35. PMID: 9833017. ↥
Lin LY, Di Stefano EW, Schmitz DA, Hsu L, Ellis SW, Lennard MS, Tucker GT, Cho AK (1997): Oxidation of methamphetamine and methylenedioxymethamphetamine by CYP2D6. Drug Metab Dispos. 1997 Sep;25(9):1059-64. PMID: 9311621. ↥ ↥ ↥
Dostalek M, Jurica J, Pistovcakova J, Hanesova M, Tomandl J, Linhart I, Sulcova A (2007): Effect of methamphetamine on cytochrome P450 activity. Xenobiotica. 2007 Dec;37(12):1355-66. doi: 10.1080/00498250701652877. PMID: 17922362. ↥
Pontes H, de Pinho PG, Fernandes E, Branco PS, Ferreira LM, Carmo H, Remião F, Carvalho F, Bastos ML (2010): Metabolic interactions between ethanol and MDMA in primary cultured rat hepatocytes. Toxicology. 2010 Apr 11;270(2-3):150-7. doi: 10.1016/j.tox.2010.02.010. PMID: 20170704. ↥
Nookala AR, Li J, Ande A, Wang L, Vaidya NK, Li W, Kumar S, Kumar A (2016): Effect of Methamphetamine on Spectral Binding, Ligand Docking and Metabolism of Anti-HIV Drugs with CYP3A4. PLoS One. 2016 Jan 7;11(1):e0146529. doi: 10.1371/journal.pone.0146529. PMID: 26741368; PMCID: PMC4704828. ↥
Kraemer T, Maurer HH (2002): Toxicokinetics of amphetamines: metabolism and toxicokinetic data of designer drugs, amphetamine, methamphetamine, and their N-alkyl derivatives. Ther Drug Monit. 2002 Apr;24(2):277-89. doi: 10.1097/00007691-200204000-00009. PMID: 11897973. REVIEW ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥
Maurer HH, Bickeboeller-Friedrich J, Kraemer T, Peters FT (2000): Toxicokinetics and analytical toxicology of amphetamine-derived designer drugs (‘Ecstasy’). Toxicol Lett. 2000 Mar 15;112-113:133-42. doi: 10.1016/s0378-4274(99)00207-6. PMID: 10720722. ↥ ↥ ↥ ↥ ↥ ↥
Delaforge M, Jaouen M, Bouille G (1999): Inhibitory metabolite complex formation of methylenedioxymethamphetamine with rat and human cytochrome P450. Particular involvement of CYP 2D. Environ Toxicol Pharmacol. 1999 Jul;7(3):153-8. doi: 10.1016/s1382-6689(99)00007-1. PMID: 21781921. ↥
Maurer H H, Kraemer T (2002): Amphetamine-derived Designer Drugs: Metabolism and Screening Procedures : Amphetamin-verwandte Designer-Drogen: Metabolismus und Screening Verfahren. , 26(1-2), 37–42. doi:10.1046/j.1439-0477.2002.02013.x ↥ ↥ ↥
Maurer HH (1996): On the metabolism and the toxicological analysis of methylenedioxyphenylalkylamine designer drugs by gas chromatography-mass spectrometry. Ther Drug Monit. 1996 Aug;18(4):465-70. doi: 10.1097/00007691-199608000-00027. PMID: 8857570. ↥ ↥
Phamarkogenetik.de: Cytochrom P450 2D6 (CYP2D6) [T88.7] Abruf 25.03.2022 ↥ ↥
Cashman JR, Xiong YN, Xu L, Janowsky A (1999): N-oxygenation of amphetamine and methamphetamine by the human flavin-containing monooxygenase (form 3): role in bioactivation and detoxication. J Pharmacol Exp Ther. 1999 Mar;288(3):1251-60. PMID: 10027866. ↥
Krueger SK, Williams DE (2005): Mammalian flavin-containing monooxygenases: structure/function, genetic polymorphisms and role in drug metabolism. Pharmacol Ther. 2005 Jun;106(3):357-87. doi: 10.1016/j.pharmthera.2005.01.001. PMID: 15922018; PMCID: PMC1828602. REVIEW ↥ ↥
Taylor KB (1974): Dopamine-beta-hydroxylase. Stereochemical course of the reaction. J Biol Chem. 1974 Jan 25;249(2):454-8. PMID: 4809526. ↥
SJOERDSMA A, von STUDNITZ W (1963): Dopamine-beta-oxidase activity in man, using hydroxyamphetamine as substrate. Br J Pharmacol Chemother. 1963 Apr;20(2):278-84. doi: 10.1111/j.1476-5381.1963.tb01467.x. PMID: 13977820; PMCID: PMC1703637. ↥
Jonsson J, Lewander T (1976): Pharmacological effects and tissue concentrations of amphetamine in rats pretreated with diethyldithiocarbamate (DDC), a dopamine-β-hydroxylase inhibitor. European Journal of Drug Metabolism and Pharmacokinetics 1, 161–166 (1976). https://doi.org/10.1007/BF03189271 ↥
Kuhn CM, Schanberg SM, Breese GR (1978): Metabolism of amphetamine by rat brain tissue. Biochem Pharmacol. 1978 Feb 1;27(3):343-51. doi: 10.1016/0006-2952(78)90238-1. PMID: 339925. ↥
Helander A, Andersson A, Villén T (2025): Origin and Interpretation of Low Methamphetamine Levels Found in Amphetamine-Positive Urine Samples: Support for Methylation of Amphetamine as a Minor Metabolic Pathway. Drug Test Anal. 2025 Nov;17(11):2276-2282. doi: 10.1002/dta.3940. PMID: 40776552; PMCID: PMC12580171. ↥
Helander A, Andersson A, Villén T (2025): Alternative routine for reporting chiral amphetamine test results in assessment of attention-deficit/hyperactivity disorder medication: experiences from 2013 to 2023. Drug Test Anal. 2025 Jan;17(1):163-169. doi: 10.1002/dta.3690. PMID: 38600633; PMCID: PMC11729626. ↥
Russell DJ, Wyrwoll CS, Preen DB, Kelty E (2024): Investigating maternal and neonatal health outcomes associated with continuing or ceasing dexamphetamine treatment for women with attention-deficit hyperactivity disorder during pregnancy: a retrospective cohort study. Arch Womens Ment Health. 2024 Mar 1. doi: 10.1007/s00737-024-01450-4. PMID: 38424254. ↥
Suarez EA, Bateman BT, Hernandez-Diaz S, Straub L, McDougle CJ, Wisner KL, Gray KJ, Pennell PB, Lester B, Zhu Y, Mogun H, Huybrechts KF (2024): Prescription Stimulant Use During Pregnancy and Risk of Neurodevelopmental Disorders in Children. JAMA Psychiatry. 2024 Jan 24:e235073. doi: 10.1001/jamapsychiatry.2023.5073. PMID: 38265792; PMCID: PMC10809143. n = 4,3 Mio ↥
Bang Madsen K, Larsson H, Skoglund C, Liu X, Munk-Olsen T, Bergink V, Newcorn JH, Cortese S, Lichtenstein P, Kuja-Halkola R, Chang Z, D’Onofrio B, Hove Thomsen P, Klungsøyr K, Brikell I, Garcia-Argibay M (2025): In utero exposure to methylphenidate, amphetamines and atomoxetine and offspring neurodevelopmental disorders - a population-based cohort study and meta-analysis. Mol Psychiatry. 2025 Mar 27. doi: 10.1038/s41380-025-02968-4. PMID: 40148550. ↥
Vitiello, B (2025): Chapter 1. Developmental Aspects of Pediatric Psychopharmacology. In Clinical Manual of Child and Adolescent Psychopharmacology (pp. 1-34) ↥
Rose, Hathcock, White, Borowski, Rivera-Chiauzzi (2020): Amphetamine-Dextroamphetamine and Pregnancy: Neonatal Outcomes After Prenatal Prescription Mixed Amphetamine Exposure. J Atten Disord. 2020 Jan 13:1087054719896857. doi: 10.1177/1087054719896857. ↥
Bro, Kjaersgaard, Parner, Sørensen, Olsen, Bech, Pedersen, Christensen, Vestergaard (2015): Adverse pregnancy outcomes after exposure to methylphenidate or atomoxetine during pregnancy. Clin Epidemiol. 2015 Jan 29;7:139-47. doi: 10.2147/CLEP.S72906. eCollection 2015. ↥
Cohen, Hernández-Díaz, Bateman, Park, Desai, Gray, Patorno, Mogun, Huybrechts (2017): Placental Complications Associated With Psychostimulant Use in Pregnancy. Obstet Gynecol. 2017 Dec;130(6):1192-1201. doi: 10.1097/AOG.0000000000002362. ↥
Haervig, Mortensen, Hansen, Strandberg-Larsen (2014): Use of ADHD medication during pregnancy from 1999 to 2010: a Danish register-based study. Pharmacoepidemiol Drug Saf. 2014 May;23(5):526-33. doi: 10.1002/pds.3600. n = 480 unter 1.054.494 Geburten ↥
Pottegård, Hallas, Andersen, Løkkegaard, Dideriksen, Aagaard, Damkier (2014): First-trimester exposure to methylphenidate: a population-based cohort study. J Clin Psychiatry. 2014 Jan;75(1):e88-93. doi: 10.4088/JCP.13m08708. ↥
Szpunar MJ, Freeman MP, Kobylski LA, Rossa ET, Gaccione P, Chitayat D, Viguera AC, Cohen LS (2023): Risk of Major Malformations in Infants After First-Trimester Exposure to Stimulants: Results From the Massachusetts General Hospital National Pregnancy Registry for Psychiatric Medications. J Clin Psychopharmacol. 2023 Jul-Aug 01;43(4):326-332. doi: 10.1097/JCP.0000000000001702. PMID: 37235505. ↥
Moran, Ongur, Hsu, Castro, Perlis, Schneeweiss (2019): Psychosis with Methylphenidate or Amphetamine in Patients with ADHD. N Engl J Med. 2019 Mar 21;380(12):1128-1138. doi: 10.1056/NEJMoa1813751. n = 221.846 ↥
Jongsma, Gayer-Anderson, Lasalvia, Quattrone, Mulè, Szöke, Selten, Turner, Arango, Tarricone, Berardi, Tortelli, Llorca, de Haan, Bobes, Bernardo, Sanjuán, Santos, Arrojo, Del-Ben, Menezes, Velthorst, Murray, Rutten, Jones, van Os, Morgan, Kirkbride; for the European Network of National Schizophrenia Networks Studying Gene-Environment Interactions Work Package 2 (EU-GEI WP2) Group(2018): Treated Incidence of Psychotic Disorders in the Multinational EU-GEI Study. JAMA Psychiatry. 2018;75(1):36–46. doi:10.1001/jamapsychiatry.2017.3554; n = 12,9 Millionen Personenjahre ↥
Gudbrandsdottir RK, Sigurdsson E, Albertsson ÞI, Jonsdottir H, Ingimarsson O (2025): Risk of hospitalisation for first-onset psychosis or mania within a year of ADHD medication initiation in adults with ADHD. BMJ Ment Health. 2025 Apr 12;28(1):e301521. doi: 10.1136/bmjment-2024-301521. PMID: 40221142; PMCID: PMC11997813. ↥
Gelbe Liste: Dexamfetamin. Abgerufen 12.02.23 ↥ ↥ ↥
Cosgrove K, Johnston CS (2017): Examining the Impact of Adherence to a Vegan Diet on Acid-Base Balance in Healthy Adults. Plant Foods Hum Nutr. 2017 Sep;72(3):308-313. doi: 10.1007/s11130-017-0620-7. PMID: 28677099. ↥
Osuna-Padilla IA, Leal-Escobar G, Garza-García CA, Rodríguez-Castellanos FE (2019): Dietary Acid Load: mechanisms and evidence of its health repercussions. Nefrologia (Engl Ed). 2019 Jul-Aug;39(4):343-354. English, Spanish. doi: 10.1016/j.nefro.2018.10.005. PMID: 30737117. REVIEW ↥
Passey C (2017): Reducing the Dietary Acid Load: How a More Alkaline Diet Benefits Patients With Chronic Kidney Disease. J Ren Nutr. 2017 May;27(3):151-160. doi: 10.1053/j.jrn.2016.11.006. PMID: 28117137 REVIEW ↥
Terrillion CE, Dao DT, Cachope R, Lobo MK, Puche AC, Cheer JF, Gould TD (2017): Reduced levels of Cacna1c attenuate mesolimbic dopamine system function. Genes Brain Behav. 2017 Jun;16(5):495-505. doi: 10.1111/gbb.12371. PMID: 28186690; PMCID: PMC5457318. ↥
Ermer J, Corcoran M, Martin P (2015): Lisdexamfetamine Dimesylate Effects on the Pharmacokinetics of Cytochrome P450 Substrates in Healthy Adults in an Open-Label, Randomized, Crossover Study. Drugs R D. 2015 Jun;15(2):175-85. doi: 10.1007/s40268-015-0090-z. PMID: 25862215; PMCID: PMC4488187. ↥
Pharmazeutische Zeitung: Lisdexamfetamin; abgerufen 10.02.21 ↥ ↥ ↥ ↥
Cooper BE, Sejnowski CA (2013): Serotonin syndrome: recognition and treatment. AACN Adv Crit Care. 2013 Jan-Mar;24(1):15-20; quiz 21-2. doi: 10.1097/NCI.0b013e31827eecc6. PMID: 23343808. ↥
Benassayag Kaduri N, Hazan A, De-Haan T, Kohn E, Berkovitch M, Berlin M (2024): Amphetamine use for attention deficit hyperactive disorder during breastfeeding and children’s neurodevelopmental outcomes: A pilot study. Psychiatry Res. 2024 Jun 17;339:116047. doi: 10.1016/j.psychres.2024.116047. PMID: 38908263. ↥
Castells, Ramon, Cunill, Olivé, Serrano (2020): Relationship Between Treatment Duration and Efficacy of Pharmacological Treatment for ADHD: A Meta-Analysis and Meta-Regression of 87 Randomized Controlled Clinical Trials. J Atten Disord. 2020 Feb 20:1087054720903372. doi: 10.1177/1087054720903372. PMID: 32075485. ↥
Schoeman R (2024): MEDICAL MANAGEMENT OF ADHD: THE LATEST TREATMENT AND MEDICATION OPTIONS FOR PATIENTS; MHM 2024, Volume 11, Issue 1 ↥