
Efficacy and Duration of Action of ADHD Medications
Only in theory is the drug concentration proportional to the administered dose. In general pharmacological practice, there are significant interindividual differences ranging from a factor of 8 to 30.1
Data from clinical trials are of little help in determining the appropriate dose of a medication for an individual. These trials examine only the dose-response relationship, but not the drug concentration. The dosages for a medication listed in prescribing information, package inserts, and textbooks are based on the average across the entire population of people with ADHD. While this information is certainly helpful as a general guide, it should not be considered the definitive standard for individual people with ADHD, who differ in many ways:1
- Gender
- Size
- Weight
- Age
- Compliance
- Liver and kidney diseases
- Comorbidities
- Interactions
- pharmacokinetic ((other) drugs)
- xenobiotic (dietary)
- Drugs (nicotine, alcohol, caffeine, recreational drugs)
- Genetics
- Metabolism gene variants
Pharmacology encompasses the fields of pharmacodynamics (what an active ingredient does to the body) and pharmacokinetics (what the body does to the active ingredient).
The most important processes in pharmacokinetics are:23
- Absorption
- Bioavailability
- Distribution
- Breakdown (metabolism)
- Excretion
In addition, the release (liberation) of the active pharmaceutical ingredient is also relevant.
There is very little universally applicable data regarding ADHD medications, their use, and their effects. While the manufacturers’ claims regarding the duration of action of methylphenidate are reasonably realistic and variations tend to be individual in nature, the stated duration of action for Vyvanse is achieved by only a small group of people with ADHD.
In the case of ADHD, however, medications must always be tested and adjusted on a highly individualized basis.
This article examines the factors that individually influence the response to and duration of action of a single dose of ADHD medication.
Although blood levels are an important factor in determining drug dosage, they cannot measure factors such as blood-brain barrier permeability or receptor activity, among others; therefore, this value alone cannot serve as an objective criterion for assessing a drug’s efficacy.
1. Duration of Action of Active Ingredients and Medications for ADHD
1.1. Manufacturer’s information on duration of action
The data for medications available in the U.S. are from Rodden.4 The figures in the table represent average values, unless otherwise noted.
The actual duration of action varies from person to person and depends heavily on the individual’s metabolism. Approximately 5% of people with ADHD are ultra-rapid metabolizers. In these individuals, due to increased CES1 activity, the effect of immediate release MPH may last only 1 hour5, or the effect of a half-day extended-release formulation may last only 1.5 or 2 hours instead of 5 to 6 hours. Similarly, although apparently less frequently, there are people with ADHD for whom a formulation has a significantly longer duration of action.
For information on the metabolism of methylphenidate and amphetamine-based medications, see below. There you will also find more detailed information on pharmacokinetics, such as the onset of action and the shape of the dose-response curve.
Especially with half-day sustained-release formulations, a second dose of medication—which is typically lower in dosage—is usually required at lunchtime to ensure full daily coverage.
Treatment for only half a day is not effective. ADHD is not a “morning disorder.”
| Methylphenidate preparations | Active ingredient | Typical duration of action in hours (according to the manufacturer) | sustained release | Country |
|---|---|---|---|---|
| Ritalin, Methylphenidate HEXAL, Methylpheni TAD (immediate release), Medikinet (immediate release), generic methylphenidate | Methylphenidate | 2.5–3.5; 3–45; 3.06 hours (2.5 to 3.875 / 1st quartile to 3rd quartile)6 | immediate release | EU, USA |
| Methylin Liquid | Methylphenidate | 3 - 4 | immediate release | USA |
| Ritalin SR | Methylphenidate | 5–8 hours duration of action (theoretical), 3–5 hours duration of action (practical)7, 84 | sustained-release7 | EU |
| Focalin | Dexmethylphenidate | 4–6 | immediate release | CH, USA |
| Equasym Retard/XL | Methylphenidate | 6–88 / 8 9 | Two-phase sustained-release | EU |
| Medikinet Adult (adults), Medikinet Retard (children) (bioequivalent)10 | Methylphenidate | 6–88; 4.65 hours (4.0 to 5.0 / 1st quartile to 3rd quartile)11 | Two-phase sustained-release | EU |
| Ritalin LA, Ritalin Adult (bioequivalent) | Methylphenidate | 6–87 / 8 8; 4.6 hours (3.38 to 6.0 / 1st quartile to 3rd quartile)12 | EU; USA: Ritalin LA only | |
| Methysym | Methylphenidate | up to 8 | sustained release | available in Germany since June 1, 2021 |
| Metadate CD | Methylphenidate | 8–10 | sustained release | USA |
| Daytrana | Methylphenidate | 10 (for a 9-hour wear time) | Patch | USA |
| Concerta, Methylphenidate Hydrochloride-neuraxpharm (bioequivalent), Methylphenidate AL Retard (bioequivalent) | Methylphenidate | 8–128, 10–127, 1213; 10.2 hours (7.5 to 11.5 / 1st quartile to 3rd quartile)14 | sustained release | Germany, Switzerland, USA |
| Focalin XR | Dexmethylphenidate | 8–12 | sustained release | CH, USA |
| Methylphenidate Hydrochloride Ratiopharm15 | Methylphenidate | 12 | sustained release | EU |
| Methylphenidate Hydrochloride Hexal16 | Methylphenidate | 12 | sustained release | EU |
| Kinecteen | Methylphenidate | 12 | sustained release | EU |
| Aptensio XR | Methylphenidate | 12 | sustained release | USA |
| Cotempla XR-ODT | Methylphenidate | 12–13 | sustained release | USA |
| Quillichew ER | Methylphenidate | 12–13 | sustained release | USA |
| Quillivant XR | Methylphenidate | 12–13 | sustained release | USA |
| Jornay PM | Methylphenidate | 12–14 | sustained release | USA |
| Amphetamine preparations | Active ingredient | Duration of action in hours (according to the manufacturer) | sustained release | Country |
|---|---|---|---|---|
| Dexedrine | Dextroamphetamine | 3–4 | immediate release | USA |
| ProCentra | Dextroamphetamine | 3–6 | immediate release | USA |
| Zenzedi | Dextroamphetamine | 3–6 | immediate release | USA |
| Desoxyn | Methamphetamine | 4–6 | immediate release | USA |
| Adderall | Amphetamine mixed salts | 4–6 | immediate release | USA |
| Evekeo | Amphetamine sulfate | 4–6 | immediate release | USA |
| Attentin | Dextroamphetamine | 5–6 | immediate release | Germany, since late 2011 |
| Dexamin | Dextroamphetamine | 5–6 | immediate release | Switzerland, as a compounded prescription |
| Dexedrine ER | Dextroamphetamine | 5–10 | sustained release | USA |
| Adderall XR | Amphetamine mixed salts | 10 - 12 | sustained release | USA |
| Adzenys ER | Amphetamine | 10–12 | sustained release | USA |
| Adzenys XR-ODT | Amphetamine | 10–12 | sustained release | USA |
| Vyvanse, Tyvanse, generic versions | Lisdexamfetamine | 13 (children); 14 (adults) (in practice, sometimes significantly lower values); 7 hours or less in 60% of people with ADHD (see below) | Prodrug | EU, USA |
| Dyanavel XR | Amphetamine | 13 | sustained release | USA |
| Mydayis | Amphetamine mixed salts | 14–16 | sustained release | USA |
| Non-stimulants | Active ingredient | Duration of action in hours (according to the manufacturer) | sustained release | Country |
|---|---|---|---|---|
| Strattera, Agakalin | Atomoxetine | all-day / individualized 8 to 21 hours17 | immediate release | USA |
| Intuniv | Guanfacine | once daily; peak concentration after approximately 5 hours; elimination half-life approximately 18 hours | sustained release | USA |
| The course of the response curves varies considerably depending on the drug.18 |
1.2. Empirical data on duration of action
1.2.1. Empirical data on the duration of action of a single dose of lisdexamfetamine
Three online surveys of people with ADHD in the German-speaking adhs-forum.adxs.org (80 participants, as of 2022), and in an English-language subreddit about Vyvanse (466 participants, through 2022), and in the ADxS Medication Duration Survey (781 participants for LDX, as of May 3, 2026), regarding how long a single dose of lisdexamfetamine (LDX, e.g., Vyvanse) lasts for them, collectively revealed:
| Duration of action of a single dose of LDX | Participants (out of 1,327) |
|---|---|
| 5 hours or less | , 31.5% |
| 6 to 7 hours | 25.8% |
| 8 to 9 hours | 19.1% |
| 10 to 11 hours | , 12.7% |
| 12 hours or more | , 11.0% |
There is a very clear trend toward a much shorter duration of action than the 10 to 12 hours specified by the manufacturer. For about one in three users, a single dose lasts only up to 5 hours, and for more than half, 7 hours or less. Fewer than a quarter of the people with ADHD experience the duration of action specified by the manufacturer—10 to 12 hours or longer. This is consistent with the numerous reports from Vyvanse users on the forum who require more than one single dose per day. Some users require 3 doses (with subsequent doses typically being lower than the preceding ones).
There is evidence that the duration of action of lisdexamfetamine is merely delayed by 1 to 1.5 hours compared to dextroamphetamine, but not prolonged.1920 This strongly calls into question the manufacturer’s claims of 12 to 14 hours per single dose and is consistent with the empirical data on the duration of action of a single dose of lisdexamfetamine Experiences of people with ADHD.
Other studies, however, show a time interval between LDX administration and peak dAMP levels ranging from 421 to 4.23 hours22 or 4.4 hours23
Impaired kidney function did not slow the breakdown of LDX, but it did slow the breakdown of dAMP, thereby prolonging its effect.24
Among the participants in the ADxS Drug Duration of Action Survey , the average single dose among the n = 391 users with a duration of action of up to 7 hours (43.6 mg) was slightly higher than the single dose among the n = 390 users with a duration of action of 8 hours or more (42.8 mg). The values showed barely any variation among adults based on age. Even among users aged 60 and older, the average dose was 38.9 mg.
The dose also did not differ significantly by weight (up to 50 kg: 42.5 mg; 51 to 70 kg: 41.9 mg; 71 to 90 kg: 43.0 mg; over 90 kg: 47.1 mg).
Interestingly, there were also several people with ADHD for whom not only Vyvanse/Elvanse but also methylphenidate had a much shorter duration of action. Since Vyvanse/Elvanse and MPH are metabolized by different enzymes, this suggests mechanisms other than overactive enzyme gene variants, as is also explained in this article.
1.2.2. Empirical data on the duration of action of a single dose of immediate release MPH
Among the participants in the ADxS Drug Duration of Action Survey (as of Dec. 19, 23), the duration of action of a single dose of immediate-release MPH was, on average, 2.95 hours (n = 20) for single doses of up to 12.5 mg (mean: 9 mg), and for single doses of 15 to 20 mg (average: 18.75 mg), it was 3.43 hours (n = 8). The overall average was 3.18 hours and 14.8 mg.
1.2.3. Empirical data on the duration of action of a single dose of MPH half-day sustained-release
Among the participants in the ADxS Drug Duration of Action Survey , the duration of action of a single dose of half-day-release MPH (Medikinet Retard, Medikinet Adult, Ritalin Adult, Ritalin LA) was 4.61 hours (n = 163). The average single dose was 21.7 mg.
| Duration of action of a single dose of MPH half-day sustained-release | Participants (out of 163) |
|---|---|
| up to 1 hour | 0.6% |
| > 1 to 2 hours | , 5.5% |
| > 2 to 3 hours | , 7.4% |
| > 3 to 4 hours | 23.9% |
| > 4 to 5 hours | 43.6% |
| 6 to 7 hours | , 14.1% |
| 8 hours or more | 4.9% |
Thus, 67.7% of people with ADHD report that a single dose is effective for 3 to 5 hours, while 81.8% report a duration of effect of 3 to 7 hours. The results are therefore significantly more consistent and closer to the manufacturer’s specifications than those for Vyvanse.
Medikinet retard and Medikinet adult (which are bioidentical) had an average duration of action of 4.58 hours (n = 132) at an average dose of 20.64 mg, Ritalin Adult and Ritalin LA (which are also bioidentical) had an average duration of action of 4.74 hours (n = 31) at an average dose of 26.3 mg.
Below, we explain the factors that can influence the duration of a medication’s effects (particularly in the case of ADHD medications) on an individual basis.
2. Single-dose amount
Some people with ADHD report that higher single doses of amphetamine (especially lisdexamfetamine) have a longer-lasting effect for them.
However, pharmacological tests of various doses of lisdexamfetamine show that Tmax is approximately the same.25 Tests with doses higher than the therapeutic dose showed that lysine cleavage is neither saturated nor slowed by higher doses.26
The duration of action of methylphenidate preparations is independent of the dose.27
3. Gastric Transit Rate
In addition to the rate of small intestine transit, gastric function also plays a role. Gastric motility and emptying rate influence how quickly a substance reaches the small intestine. For example, with acetaminophen, gastric emptying is the rate-limiting step for the substance’s appearance in the blood plasma. Delayed or accelerated gastric emptying can therefore fundamentally influence the kinetics of orally administered medications, so that, for example, the necessary therapeutic levels are not reached or are reached only after a delay.28
With age, the surface area of the small intestine and the rate of gastric emptying decrease. At the same time, the pH of the stomach increases. However, these changes usually have no effect on drug absorption.2930
Anticholinergic drugs can slow the passage of medications from the stomach into the small intestine.2930
Gastric bypass surgery or gastric reduction surgery increased dexamfetamine levels when lisdexamfetamine was administered. Tmax tended to be reduced. For Ritalin acid (from MPH) and atomoxetine, no changes in AUC0-24 were observed; atomoxetine showed a higher Cmax and a shorter Tmax. The number of subjects was very small.31
4. Small intestine
4.1. Small Intestine Length
In children, the small intestine is shorter, resulting in reduced absorption through the small intestine.3233
4.2. Small Intestine Transit Time
“For oral medications, the transit time through the stomach and small intestine represents a natural upper limit for the release of the active ingredient: Once the tablet has left the small intestine, nothing more can be absorbed, so the release is limited to a period of about 8–10 hours.”34
This time can vary from person to person, just as the speed of intestinal transit varies. This is likely the reason why there are a few people with a very fast metabolism who report that Medikinet lasts 1 to 2 hours and Vyvanse lasts 3 hours. They also report that they need to eat much more frequently throughout the day than others.
To achieve a duration of action that is longer (not just on average) than intestinal transit time, mechanisms are therefore required that go beyond absorption from the small intestine.
5. Acid-base balance
pH is the abbreviation for “potentia hydrogenii” and is a logarithmic measure of the proton concentration (H+ or H3O+) in an aqueous solution. The more protons there are in a solution, the lower the pH value.
The pH scale ranges from 0 to 14 and indicates how alkaline something is. 7 is neutral. The higher the pH (above 7), the more alkaline it is; the lower the pH (below 7), the more acidic it is.
The typical pH value is:
- e in the stomach35
- on an empty stomach, pH 1.5 (1–2)
- increases when eating
- depending on the type and amount, up to a pH of 5–6
- followed by a decline back to the initial value
- Preterm infants have less acidic stomachs (pH > 4) and are prone to intestinal infections
- Older adults have lower stomach acidity (pH 6.6 in 80% of study participants) and are susceptible to bacterial infections in the stomach and intestines
- Stomach acid (hydrochloric acid) is produced in parietal cells by the proton pump
- That is why proton pump inhibitors reduce stomach acid (omeprazole, lansoprazole, rabeprazole, esomeprazole, pantoprazole)
- Excess acids are neutralized by buffer systems and excreted through respiration and the kidneys
- in the urine36
- 6.0 Average
- 6.6 and higher in 10% of people
- 7.2 and higher at 1%
Depending on the duration of exposure to acid, the pH value can affect:35
- Solubility of active ingredients
- Stability of active ingredients
Foods affect the body’s pH level.37
Foods high in animal protein (meat, fish, cheese, eggs) produce acids as metabolic byproducts.
Plant-based foods (fruits, vegetables, leafy greens, whole-grain products) are primarily alkaline.
5.1. Acid-Base Balance and Amphetamine Medications
Amphetamine-based medications:
The amount of dextroamphetamine that is excreted unchanged—and thus the amount of pharmacologically active dextroamphetamine that remains—depends on the pH of the urine.38394041
- Reduced duration of action due to high urinary acidity (low pH), e.g., caused by (see detailed list below)
- Ascorbic acid (vitamin C)41
- Ascorbic acid (vitamin C) taken in an appropriate dose left the pH value virtually unchanged (+0.03)42
- Vitamin C (ascorbic acid) is rapidly metabolized, and its PRAL value (potential renal acid load) is close to zero (= neutral). However, high doses of vitamin C can temporarily acidify the urine because excess ascorbic acid is excreted by the kidneys and can lower the pH of the urine. This applies to high doses taken as dietary supplements, but barely to normal dietary intake.
- Thiazide diuretics
- A diet rich in animal protein
- Diabetes
- respiratory acidosis
- Ascorbic acid (vitamin C)41
- Prolonged duration of action due to low (alkalized) urinary acidity (high pH)20, e.g., through (see detailed list below)
- Potassium citrate
- Sodium hydrogen carbonate = sodium bicarbonate
- Mineral water with bicarbonate43
- A diet rich in fruits, vegetables, and whole grains
- Urinary tract infections
- Vomiting
- A change in diet, e.g., from a meat-based diet to a vegetarian diet44
- heavy use of medications to neutralize stomach acid44
A urine pH of 5.0 (acidic) can reduce the pharmacologically active amount of d-AMP to one-quarter of the amount at a urine pH of 8.0 (alkaline).45 AUC of amphetamine after a 11 mg dose at a urine pH of:
- pH 5.0: 361 µg·h/L
- pH 6.5: 692 µg·h/L
- pH 8.0: 1325 µg·h/L
The highest available value for the pharmacological concentration of d-AMP (Cmax) also correlates with urine pH, albeit to a much lesser extent; thus, acidic urine correlates with a slightly weaker effect, but above all with a significantly shorter duration of action.38
While 54.5% of orally administered amphetamine was excreted unchanged at pH = 5.0 (acidic urine), this value was 2.9% at pH = 8 (alkaline urine). When the pH was uncontrolled, 14.5% was excreted.3845
A person with ADHD for whom lisdexamfetamine’s effects were too short-lived (a single 50-mg dose lasted 4 hours) reported that drinking 1.5 liters of sparkling water containing 1,800 mg nhc/L in the morning enhanced the effect to such an extent that he now only needed 30 mg of LDX, which then had the same intensity and duration of effect as the previous 50 mg dose.
5.2. Acid-Base Balance and Methylphenidate
In a laboratory study (= in vitro), up to 60% of the methylphenidate was spontaneously hydrolyzed to (pharmacologically inactive) ritalinic acid, and this hydrolysis was pH-dependent.46
In bacterial cultures in which MPH was not metabolized, the pH after 24 hours ranged from 4.0 to 5.5; in cultures with high MPH hydrolysis, the pH ranged from 7.5 to 8.0. E. coli BW25113 cultures with an average pH of 7.8 hydrolyzed 70% of the MPH; E. coli DSM1058 and E. coli DSM12250, with an average pH of 7.6, hydrolyzed 50% of the MPH. The correlation between MPH-hydrolyzing bacterial cultures and the pH of the bacterial cultures after 24 hours was very high (r = 0.89, r² = 0.79, p-value = 0.0006). In pure culture medium, less than 20% of the MPH was hydrolyzed to ritalinic acid at a pH of 6.0, and 80% at a pH of 8.0. Bacteria did not contribute to the metabolism of MPH.46
In adults, only 22% (+/- 8%) of dMPH and 5% (+/- 3%) reach the systemic circulation; in children, the figures are 31% (+/- 16%).47 Schematically, 20% of MPH is oxidized in the liver.48 80% of ingested MPH is excreted in the urine within 48 hours (of which 80% is in the form of Ritalin acid and 1% is unmetabolized), and 3% is excreted in the feces. 47
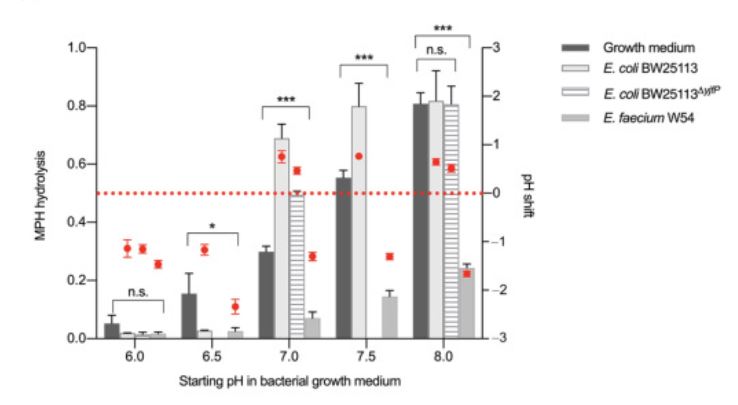
Source: Aresti-Sanz J, Schwalbe M, Pereira RR, Permentier H, El Aidy S (2021): Stability of Methylphenidate under Various pH Conditions in the Presence or Absence of Gut Microbiota. Pharmaceuticals (Basel). July 27, 2021;14(8):733. doi: 10.3390/ph14080733. PMID: 34451830; PMCID: PMC8398889 (unchanged)46 Published under the terms of the Creative Commons Attribution (CC BY)license.
According to these laboratory results for MPH, a high pH value should be associated with a reduced MPH effect. This would be in direct contrast to the shortened amphetamine effect, which has also been empirically (= in vivo) confirmed at low urine pH levels. It remains to be seen whether the study results for MPH will be empirically confirmed. Since MPH, like amphetamine, is slightly basic, the results regarding MPH also contradict general pharmacological experience. Furthermore, this would not explain the purely empirically observed simultaneous shortening of the duration of action of amphetamine medications and MPH preparations in some people with ADHD, for which no comprehensible mechanism has yet been identified.
Medikinet Retard, Medikinet Adult:
If the stomach pH is above 5.5, dose-dumping phenomena may occur with Medikinet retard and Medikinet adult: The active ingredient is released too quickly, resulting in increased effects and side effects. This can be caused by, among other things,
- Proton pump inhibitors (e.g., pantoprazole, omeprazole)
- Antacids
- H2 blockers (e.g., ranitidine, famotidine) (less likely)
- age-related increase
- atrophic gastritis
A person with ADHD reported that Medikinet had barely any effect at doses ranging from 20 to 60 mg. Eating dry rice cakes in addition to the medication produced a temporary effect that was unpredictable. Taking antacids (stomach acid inhibitors) in addition to MPH produced a reliable effect.
Ritalin for adults:
Ritalin for adults, on the other hand, releases MPH regardless of pH. The prescribing information lists reduced absorption as a likely interaction with antacids.50
5.3. Acid-Base Balance and Memantine
Memantine:
- Prolonged effect due to alkaline urine
- In patients with alkaline urine (high pH), the renal clearance of memantine may be reduced by a factor of 7 to 9.44
5.4. Factors that increase alkalinity (raise the pH)
Information in the following list that does not include its own source citation is taken from 51. The website cited there as the source is no longer accessible. The information has proven to be incorrect in several cases and should therefore be verified individually.
Factors that contribute to alkaline urine (high pH) include:
- Environmental factors:
- Daily fluctuations
- There are various profiles, though:36
- “Normal” pH curve with three peaks corresponding to morning and postprandial (after-meal) fluctuations, with a low nighttime pH value
- Meals cause a spontaneous increase in alkalinity (urine pH reaches at least 6.8 1 to 2 hours after meals)
- A consistently low pH level with no real fluctuations
- A single afternoon peak with an almost complete absence of morning fluctuations
- Reversal of the “normal” curve, with a low daytime level and a high nighttime plateau
- “Normal” pH curve with three peaks corresponding to morning and postprandial (after-meal) fluctuations, with a low nighttime pH value
- There are various profiles, though:36
- Body surface area (unclear whether high or low)52
- Cadmium Exposure
- Heparin
- Reduced air pressure; hypobaric ventilation53
- Mercury pollution
- Female gender5455
- Age: Stomach acid decreases, while uric acid levels rise steadily (at least in people with kidney stones) with age5655
- Low income5758 (socioeconomic status?)
- Storing the urine at too high a temperature after collection51
- Daily fluctuations
- Diseases:
- 21-Hydroxylase Deficiency
- 3-Hydroxydehydrogenase Deficiency
- Rejection of a Kidney Transplant
- Acute Poststreptococcal Glomerulonephritis
- Amyloidosis
* atrophic gastritis (age-related gastritis) - Calcium Deficiency36
- Carbonic Anhydrase II Deficiency
- Chronic Obstructive Pulmonary Disease
- Vomiting
- Acquired adrenal insufficiency
- Familial Methyl Oxidase Deficiency
- Galactosemia
- Gout
- Glycogen storage disease
- Urine dilution36
- Increased urine flow36
- Hereditary Fructose Intolerance
- Hyperventilation36
- Hypoxia59
- Lactosuria
- Light-Chain Multiple Myeloma
- Lowe Syndrome
- Lupus nephritis
- Malabsorption
- Medullary cystic disease
- Metabolic alkalosis
- Metachromatic leukodystrophy
- Mineralocorticoid deficiency, transient in infancy
- Wilson’s disease
- Multiple Myeloma
- Kidney Transplant
- Renal vein thrombosis
- Obstructive nephropathy
- Pseudohypoaldosteronism
- Renovascular Hypertension
- Salt-loss nephritis
- Sjögren’s Syndrome
- Tubulointerstitial disease
- Tyrosinemia
- Vitamin D Deficiency
- Vitamin D Resistance
- Medications:
- Acetazolamide: Increase in urine pH of +2.0 with intravenous administration (very strong); +0.39 (weak) with oral administration42
- Long-term treatment with acetazolamide has been associated with an increased risk of urolithiasis60
- ADV7103 (Citrate + Bicarbonate): Increase in urine pH by +1.27 (marked)42
- Ambroxol61
- Amiloride
- Aminoglycosides
- Ammonium chloride
- Antibiotics62
- Ascorbic acid (vitamin C): Increase in urine pH by +0.03 (neutral)42
- Bicarbonates (= hydrogen carbonates)
- Mineral water rich in bicarbonate63
- Bicarbonate loading (soda loading, baking soda loading): Increase in urine pH by +1.44 (very significant)42
- Consumption of sodium bicarbonate (= sodium hydrogen carbonate, baking soda, bicarbonate of soda, baking powder, Bullrich salt)
- 10 minutes before physical activity
- Dose: 0.2 to 0.3 g/kg
- One teaspoon of baking soda dissolved in a glass of still water
- Should not be used for more than 2 weeks
- Long-term use may trigger increased stomach acid production as a counter-reaction
- Baking soda in the stomach produces CO2—risk of stomach wall distension
- Citrate: 0.61 (moderate)4263
- Citrus juices
- Orange juice: Increase in urine pH of +0.68 (moderate)42
- Citro-Soda: Increase in urine pH by +1.56 (very strong)42
- Ingredients: Sodium bicarbonate 1.716 g, sodium citrate 0.613 g, citric acid 0.702 g, tartaric acid 0.858 g
- Cholestyramine
- Converting Enzyme Inhibitors
- Corticotropin
- Coumarin
- Diazoxide
- Exenatide: Increase in urine pH by +0.51 with intravenous administration (moderate)42 (diabetes medication)
- Glycine: Increase in urine pH by +0.20 (neutral)42
- Indomethacin: Increase in urine pH by +1.0 (marked)42
- Potassium citrate42
- Recommendation from the American Urological Association (AUA) on Increasing Urine pH
- Food additive E332
- Dietary supplements, available over the counter in powder or capsule form
- Avoid in cases of hyperkalemia—therefore, always consult a doctor; the prevalence of hyperkalemia in the general population is 2 to 3%
- Potassium gluconate: Increase in urine pH by +0.46 (mild)42
- Potassium gluconate, a medication for potassium deficiency
- Potassium hydrogen carbonate (potassium bicarbonate): Increase in urine pH by +0.89 (moderate)4264
- Potassium sodium hydrogen carbonate (also known as potassium sodium hydrogen citrate)65
- Medication to increase urine pH
- L-tryptophan: Increase in urine pH by +0.20 (neutral)42
- Magnesium salts without chlorides66
- Metolazone
- Monosodium Glutamate67
- Sodium hydrogen carbonate (sodium bicarbonate, baking soda): Increases urine pH by +1.19 when taken orally; +1.12 when administered intravenously; strong42
- Sodium L-ascorbate with sodium saccharin68
- Niacin
- Omeprazole (proton pump inhibitor): Increase in urine pH by +0.10 (neutral)42
- Spironolactone
- Streptozocin
- Topiramate: Increase in urine pH by +0.45 (mild)42
- Acetazolamide: Increase in urine pH of +2.0 with intravenous administration (very strong); +0.39 (weak) with oral administration42
- Food
- DASH Diet: Increase in urine pH of +0.5 (moderate)42
- A diet rich in fruits, vegetables, whole grains, low-fat dairy products, fish, poultry, nuts, and seeds
- Cucumbers: Increase in urine pH by +0.17 (neutral)42
- Potatoes: Increase in urine pH of +0.28 (slight)42
- Lime Juice: Increases urine pH by +0.25 (neutral)42
- It is unclear whether “lime syrup” refers to a mixture of lime juice, water, and sugar or to pure lime juice.
- Melon juice: Increases urine pH by +0.36 (cantaloupe; slight)42; higher than orange juice (moderate)69
- Milk: Increase in urine pH of +0.36 (slight)42
- Fruit and vegetable-rich diet: Increase in urine pH of +0.35 (slight)42
- Orange juice: Increase in urine pH of +0.68 (moderate)42
- French fries: Increase in urine pH by +0.25 (neutral)42
- Vegetarian diet
- Vitamin C: Increase in urine pH by +0.03 (neutral)42
- See below (PRAL value table)
- DASH Diet: Increase in urine pH of +0.5 (moderate)42
5.5. Factors that increase acidity (lower the pH)
Information in the following list that does not include its own source citation is taken from 51. The website cited there as the source is no longer accessible. The information has proven to be incorrect in several cases and should therefore be verified on a case-by-case basis.
Factors that contribute to acidic urine (low pH) include:
- Environmental factors:
- Bed rest
- Aldosterone
- Lead exposure70
- Cadmium71
- Toluene
- Vanadium
- Age: Stomach acid decreases, while uric acid levels rise steadily (at least in people with kidney stones) with age 5655
- Male gender54
- High income5758 (socioeconomic status?)
- Physical exertion in a hot environment
- Sleep deprivation: -0.0 (neutral)42
- Diseases:
- Breathing problems
- Obstruction of the airways or impairment of gas exchange in the lungs, e.g., in cases of pulmonary edema (fluid in the lungs)
- Pneumonia
- Loss of functional lung tissue, e.g., due to tuberculosis
- Insufficient respiratory drive, such as in cases of sleeping pill poisoning
- Paralysis of the respiratory muscles, e.g., in polio
- Dysfunction of the respiratory reflexes
- Adrenal Hyperfunction
- Adrenal insufficiency
- Amyloidosis
- Autoimmune Thyroiditis
- Balkan Nephropathy
- Chronic active hepatitis
- Chronic Kidney Disease
- Chronic Kidney Disease
- Chronic Pyelonephritis
- Cystinosis
- Diabetes mellitus
- Distal renal tubular acidosis
- Gastrinoma
- Zollinger-Ellison syndrome, a rare pancreatic tumor
- Increases stomach acid
- Fibrosing alveolitis
- Urinary tract obstruction (a blockage in the urinary system that prevents urine from flowing from the kidneys to the urethra)
- Helicobacter pylori infection
- Increases stomach acid
- Hepatolenticular Degeneration
- Hereditary Fructose Intolerance
- Idiopathic hypercalciuria
- Hypergammaglobulinemia
- Hyperparathyroidism
- Increased stomach acid in 30% of people with ADHD
- Cryoglobulinemia
- Fabry disease
- Wilson’s disease
- Marfan Syndrome
- Medullary Spongy Kidney
- Metabolic Acidosis
- Metabolic Syndrome76
- Kidney transplant rejection
- Kidney failure
- Polyarteritis nodosa
- Primary biliary cirrhosis
- Proximal renal tubular acidosis (Type II)
- Sickle Cell Anemia
- Sjögren’s Syndrome
- Voltage-dependent distal renal tubular acidosis (Type 1)
- Vitamin D Toxicity
- Breathing problems
- Medications:
- Acetaminophen = Paracetamol
- Acetazolamide
- Amiloride
- Ammonium chloride (sal ammoniac): - 1.63 (very strong)4238
- Amphotericin B
- Acetylsalicylic acid (Aspirin)
- Inhibits prostaglandins, which protect the stomach lining from acid
- A prostaglandin deficiency leads to inflammation of the mucous membrane, which damages the parietal cells that produce stomach acid (gastritis)
- Carbenoxolone
- Cefdinir
- Cimetidine
- Citric acid: Reduces urine pH by -0.06 (neutral)42
- Dapagliflocin: Decrease in urine pH by -0.10 (neutral)42 (diabetes medication)
- Diclofenac
- Inhibits prostaglandins, which protect the stomach lining from acid
- Prostaglandin deficiency leads to inflammation of the mucous membrane, which damages the parietal cells that produce stomach acid (gastritis) * Diflunisal
- Etodolac
- Fenoprofen
- Flurbiprofen
- Furosemide: Decrease in urine pH by -0.52 following intravenous administration (not statistically significant)42
- Ibuprofen
- Inhibits prostaglandins, which protect the stomach lining from acid
- A prostaglandin deficiency leads to inflammation of the mucous membrane, which damages the parietal cells that produce stomach acid (gastritis)
- Ifosfamide
- Indomethacin
- Ketoprofen
- Lithium
- Mafenid
- Methionine: Decrease in urine pH by -0.71 (moderate)42
- Essential amino acid
- Over-the-counter
- Takes a few days to take effect
- Monomagnesium L-aspartate hydrochloride66
- Mefenamic acid
- Naproxen
- Niacinamide
- Ofloxacin
- Orthophosphate
- Parathyroid Extract
- Proton pump inhibitors: Decrease in urine pH by -1.5 (very strong, n = 10)49
- Ranitidine
- Triamterene
- Food
- Apple cider vinegar: Decrease in urine pH of -0.21 (very slight)42
- Cranberry: Decrease in urine pH by -0.16 (neutral)42
- Protein: high intake of animal protein in the diet77
- Fasting: Decrease in urine pH of -1.2 (very significant)42
- Fructose: Decrease in urine pH by -0.26 (very slight)42
- Sodium chloride (table salt): Decrease in urine pH by -0.47 (mild)42’
- Ketogenic diet: Decrease in urine pH of -0.55 (moderate)42
- Low-oxidant diet: Decrease in urine pH by -0.10 (neutral)42
- High-protein diet: Decrease in urine pH of -0.65 (moderate)42
- See below (PRAL value table)
5.6. The Effect of Food on Acid-Base Balance (PRAL Value)
Foods can significantly influence the body’s pH level. It is not so much the sour taste that matters, but rather the PRAL value. Consuming foods with a negative PRAL value correlates with an alkaline urine pH, while an acid-forming diet correlates with alkaline urine pH values below 6.0. The blood pH level in healthy adults ranges between 7.35 and 7.45.
You can measure your urine pH yourself using simple pH test strips available at drugstores or online. Fats and carbohydrates do not normally affect the acid-base balance.
When it comes to proteins, a distinction must be made between plant-based and animal-based proteins. After 7 days on a vegetarian diet, the urine pH rises and the PRAL value decreases; the same is true for a vegetarian diet of 2 or 3 days per week.78 A vegetarian diet is thus associated with a prolonged effect of amphetamine-based medications.
Foods high in oxalate can increase acid production.43
A study provides the following calculation formula:79 PRAL (mEq/d) = 0.49 × Protein (g/d) + 0.037 × Phosphorus (mg/d) − 0.021 × Potassium (mg/d) - 0.026 × magnesium (mg/d) - 0.013 × calcium (mg/d).
In other words: Foods with a strongly negative PRAL value result in alkaline urine (less acidic, increasing the pH) and thus promote a prolonged effect of amphetamine medications. Foods with a high PRAL value result in acidic urine (lowering the pH) and thus promote a shorter duration of action for amphetamine medications. According to this model, hard cheese is suitable for shortening the effects of amphetamine medications, while raisins could prolong them.
Note: Do not confuse the PRAL value with the increase in urine pH shown in the figure above. These values are inversely related.
Food PRAL Value Table
| Foods (unsweetened, untreated) | PRAL value per 100 g (A negative PRAL value increases the pH, making urine more alkaline. A positive value decreases the pH, making urine more acidic) |
|---|---|
| Sodium bicarbonate, baking soda | is highly alkaline |
| Dried chanterelles | -61.980 |
| Cocoa powder, heavily defatted | -4980 |
| Beet syrup/sugar beet molasses | -31.680 |
| Agar | -25.580 |
| Apple Pectin | -21.480 |
| Dried apricots | -21.280 |
| Raisins | -21.081 |
| Banana chips (dried banana) | -19.680 |
| Tomato Paste -19.480 | |
| Dried figs | -18.1 |
| Spinach | -14.081 |
| Prunes -12.380 | |
| Parsley | -12.0 |
| Dried kidney beans | -1280 |
| Raw spinach | -11.843 |
| Soy flour | -11.580 |
| Carob flour | -11.580 |
| Guar gum | -11.580 |
| Potato starch | -11.580 |
| -11.5 Dark Chocolate | |
| Apple concentrate/fruit syrup | -11.280 |
| Assorted Dried Fruit | -10.380 |
| Dried dates | -10.180 |
| Beans, white, dried | -9.980 |
| Dried onions | -9.780 |
| Spinach Leaves | -9.780 |
| Dried apple rings | -9.680 |
| Dried pineapple | -9.680 |
| Potatoes | -8.543 -4.079 stored -4.081 |
| Avocado | -8.580 |
| Soy Bread | -880 |
| Kale | -8.043 |
| Fennel | -7.9 |
| Swiss chard | -7.680 |
| Arugula | -7.5 |
| Beans | unclear: -7.443 or 1.143 |
| Chestnuts, pre-cooked and vacuum-sealed | -7.480 |
| Basil | –7.3 |
| Parsnip | -7.280 |
| -7.1 radish80 | |
| Bananas | -6.943 |
| Kale | -6.880 |
| Lamb’s lettuce | -6.6 |
| Blackcurrant | -6.581 |
| Lamb’s lettuce | -680 |
| Beets | -5.980 |
| Brussels sprouts | -5.780 |
| Carrots, raw | -5.743 young -4.981 |
| Kiwi | -5.643 -4.181 |
| Chives | -5.3 |
| Celery | -5.043 -5.281 |
| Apricots | -4.881 |
| Carrot juice | -4.8 |
| Zucchini | -4.681 |
| Lettuce | -4.343 -2.581 |
| Mushrooms | -4.243 -1.481 |
| Tomatoes | -4.143 -3.181 |
| Radishes | -3.781 |
| Orange juice | -3.743 -2.981 |
| Oranges | -3.643 -2.781 |
| Broccoli | -3.643 -1.281 |
| -3.5 Fruit Tea43 | |
| Grapefruit | -3.243 -1.081 |
| Green beans | -3.181 |
| Cherries | -3.143 3.681 |
| Mango | -3.043 |
| Soya | -2.943 |
| Pears | -2.981 |
| Tomato Juice -2.881 | |
| Hazelnuts | -2.881 |
| Pineapple | -2.781 |
| Strawberries | -2.543 -2.281 |
| Cucumbers | -2.443 -0.881 |
| Peaches | -2.481 |
| Lemons | -2.343 Lemon juice -2.581 |
| Red wine | -2.243 -2.47981 |
| Asparagus | -2.243 |
| Regular Spaghetti | -2.243 6.581 8.079 |
| Unsweetened apple juice | -2.281 |
| Chicory | -2.081 |
| Watermelon | -2.043 -1.981 |
| Onions | -2.043 -1.581 |
| Eggplant | -2.043 -3.481 |
| Apples | -1.943 -2.281 |
| Hazelnuts | -1.943 |
| Leek | -1.881 |
| Apollinaris Mineral Water | -1.881 |
| Iceberg Lettuce | -1.681 |
| -1.5 Jam81 | |
| Coffee (beverage) | -1.481 |
| Green bell pepper | -1.481 |
| Cauliflower | -1.343 -4.081 |
| Milk Chocolate -1.3 | |
| White Wine -1.2 dry, -1.24381 | |
| Mineral Water -0.843 | |
| Margarine | -0.843 -0.581 |
| Soy Milk -0.6 | |
| Chocolate milk | -0.643 -0.481 |
| Asparagus | -0.481 |
| Honey | -0.381 |
| Tofu | -0.3 |
| Indian tea (beverage) | -0.381 |
| Green Tea | -0.343 |
| Draft Beer -0.281 | |
| -0.243 | |
| Volvic Mineral Water | -0.181 |
| Strong Beer -0.181 | |
| White sugar | -0.181 |
| Olive oil | 04381 |
| Sunflower oil | 04381 |
| Butter | 0.143 0.681 |
| Milk (whole milk, skim milk) | 0.243 0.779 1.1 81 pasteurized UHT milk 0.781 |
| Cola | 0.243 0.481 |
| Buttermilk | 0.581 |
| , 0.6 Milk Ice Cream81 | |
| Full-bodied beer, light | 0.981 |
| Beans | unclear: 1.143 or -7.443 |
| Peas | 1.281 |
| Sour cream, fresh | 1.281 |
| Fruit Yogurt 1.281 | |
| , 1.5 Natural Yogurt81 | |
| Rice, cooked | 1.681 |
| Whole-wheat bread | 1.881 |
| Pistachios | 2.043 |
| Almonds | 2.043 |
| Chicken egg white | 2.143 1.181 |
| Lenses | 2.143 3.581 |
| Rice, unhusked | 2.343 |
| Milk Chocolate 2.481 | |
| Chickpeas | 2.643 |
| Biscuit | 3.079 |
| Rye crispbread | 3.381 |
| Madeira Cake | 3.781 |
| White bread | 3.77981 |
| ’s Mixed-Grain Bread 3.881 | |
| Rye-Wheat Bread | 4.081 |
| Rye Bread | 4.181 |
| Rice, hulled, raw | 4.579 4.681 |
| Corn tortilla | 4.843 |
| Greek yogurt | 5.343 |
| Pork Sausage 5.843 | |
| Rusks 5.9 | |
| Whole-Grain Rye Flour 5.981 | |
| White bread | 6.079 |
| Cornflakes | 6.081 |
| Peanuts | 6.243 |
| Egg Noodles | 6.481 |
| Viennese Sausages / Frankfurt Sausages | 6.781 |
| Walnuts | 6.881 |
| Haddock | 6.881 |
| Wheat flour, extract | 6.981 |
| Hering | 7.081 |
| Wheat tortilla | 7.243 |
| Whole-Wheat Spaghetti 7.381 | |
| Spelt (green spelt, whole grain) | 7.5 |
| Shrimp | 7.6 |
| Cottage cheese | 7.943 8.781 |
| Meat | 8.082 |
| Fish | 8.082 |
| Sheep Cheese 8.280 | |
| Peanuts, unsalted | 8.381 |
| Whole-grain wheat flour | 8.481 |
| ’s rump steak 8.881 | |
| Chicken egg (whole egg) | 9.043 8.281 4.079 |
| Pine Nuts | 8.880 |
| , Kasseler 8.880 | |
| Quinoa, raw | 8.980 |
| Veal Fillet | 9.081 |
| Salmon | 9.180 |
| Redfish | 9.180 |
| Schnitzel, Pork | 9.380 |
| Blue cheese | 9.380 |
| Duck | 9.580 |
| Cornmeal, Whole Grain | 9.680 |
| Turkey meat | 9.981 |
| Roquefort | 1080 |
| Hering | 10.180 |
| Lunch Special | 10.281 |
| Sunflower seeds | 10.380 |
| Mozzarella | 10.480 |
| Turkey | 10.580 |
| Smoked Salmon 10.580 | |
| Liver Sausage 10.6 81 | |
| Yeast | 10.680 |
| Oatmeal (whole grain) | 10.781 |
| Brown trout, steamed | 10.881 |
| Veal liver, raw | 10.980 |
| Shrimp | 11.180 |
| Vegetable broth, granulated (powder) | 11.180 |
| Quark | 11.181 |
| Salami | 11.681 |
| Pumpkin seeds | 11.380 |
| Macadamia nuts | 11.580 |
| Lamb | 1280 |
| Einkorn flour | 1280 |
| Cream Cheese 12.443 | |
| Brown Rice | 12.581 |
| Beef | 12.543 lean 7.881 |
| Edam | 13.180 |
| Shrimp | 13.243 |
| Corned beef | 13.281 |
| Mountain Cheese 13.380 | |
| Butterkäse | 13.780 |
| Nuts | 13.843 |
| Sponge Cake | 13.880 |
| Salmon | 14.043 |
| Veal liver | 14.2 |
| Pork | 14.743 lean 7.981 |
| Beef liver | 14.780 |
| Camembert | 15.082 14.681 |
| Mussels | 15.243 |
| , 15.5 | |
| Oil-packed sardines | 15.943 |
| Brazil nuts | 1680 |
| Chicken | 16.543, 11.8180, 8.781 |
| Flaxseeds | 17.380 |
| Chicken egg yolk | 18.143 23.481 |
| Cod | 19.843 Fillet 7.181 |
| Gouda | 20.043 18.681 |
| Cheddar | 20.079 |
| Hemp seeds, hulled | 21.3480 |
| Emmentaler | 21.5 |
| Parmesan | 21.443 34.281 |
| Gruyère | 23.3280 |
| Cheddar, low-fat | 26.481 |
| Baking powder (sodium bicarbonate + acid + anti-caking agent) | 297.9980 |
6. Mechanical Effects of Food Intake
6.1. Food Intake as a Prerequisite for the Extended-Release Effect of Medikinet
For Medikinet Adult and Medikinet Retard, prior or simultaneous food intake is a prerequisite for the sustained release of the active ingredient. If no food is consumed, the MPH is released twice as fast. Consequently, the released dose of MPH is approximately doubled, and the duration of action is approximately halved.
Other sustained-release formulations use different mechanisms for sustained release of the active ingredient that do not depend on simultaneous food intake, such as
- Ritalin for adults
- Ritalin LA
- Methysym
- Equasym Retard/XL
- Methylphenidate Hydrochloride - Neuraxpharm
- Kinecteen
- Methylphenidate Hydrochloride Ratiopharm
- Methylphenidate Hydrochloride Hexal
6.2. Food intake affects the duration of action
Regardless of the need for a delayed-release effect in some MPH formulations and regardless of the influence on urine pH (in the case of amphetamine medications) or gastric pH (in the case of MPH), certain patterns of food intake influence the effects and duration of action of stimulants in a more mechanical manner.
When taken with a high-fat meal, lisdexamfetamine (Vyvanse) reaches its peak blood level one hour later (4.7 hours instead of 3.8 hours after administration).83 However, other parameters, such as the duration of action, remain unchanged.
One person with ADHD shares their story:
“I’ve been taking Medikinet Adult consistently for three months now, and it took me a long time to find the right regimen for me. In addition to the dosage (20-10-0 for me), other factors related to food intake have also been important for me. Eating too much while taking it is a problem for me, as is eating too little. And I get better results when I eat something high in carbohydrates along with the medication.”
6.3. Food intake delays the peak AMP level
When taken with a high-fat meal, lisdexamfetamine (Vyvanse) reaches its peak blood level one hour later (4.7 hours instead of 3.8 hours after administration).83 However, other parameters, such as the duration of action, remain unchanged.
6.4. Absorption of the active ingredient
Some foods have the ability to absorb active ingredients, thereby delaying the onset and duration of their effects.
Example:
- Psyllium seeds8485 , which is why it is recommended to wait half an hour to one hour before taking other medications86
7. Physical Activity / Sports
Some people with ADHD report that intense sports can shorten the duration of stimulants by up to 40%.87
8. Nicotine / Smoking
Several people with ADHD reported that smoking altered the effects of stimulants.
The following were reported (in each individual case as a specific occurrence associated with stimulant use):
- A person with ADHD shares:
- Increased nicotine cravings 4 hours after taking Vyvanse
- After the first cigarette of the day, I feel a bit sluggish and start to get tired
- A day without cigarettes and just taking Vyvanse is going okay, except for the restlessness caused by nicotine withdrawal, but I’m still motivated and feeling the effects through the afternoon and into the evening
- Switching to nicotine “gum” instead of smoking or vaping resulted in significantly greater calm and an end to midday fatigue
- One person with ADHD described an effect similar to drug dependence:
- Vyvanse + nicotine: reduced effectiveness, negative feelings
- MPH + nicotine: enhanced effect, “kick” (but also a greater drop/rebound)
- An occasional smoker:
- Even just one or two cigarettes can prevent Vyvanse and MPH from working properly
- It takes a few days for them to start working properly again
- I usually sleep well with Vyvanse these days. When I’ve smoked, I sleep worse.
- The difference in how Vyvanse works when I haven’t smoked for a while is enormous
- A person with ADHD:
- When I take on too much, I feel the urge to smoke—either as a way to cope or as a way to push myself further.
- It works at first, but after a few days, things take a turn for the worse. I start to feel less energetic, and my mood gets worse.
- In the long run, it’s not good for me, and it doesn’t mix well with my medication. The medication becomes less effective, and in the end, I feel worse.
- A female steamship passenger:
- After taking MPH, vaping makes me feel tired and gives me a headache
- Nicotine enhances the effects of MPH
9. Alcohol
Alcohol can increase amphetamine levels.88
10. Cycle
The female menstrual cycle affects dopamine levels. Estrogen influences COMT, which breaks down dopamine in the PFC.
People with ADHD who have certain COMT gene variants are particularly susceptible.
The required dose of stimulants may vary depending on the phase of the cycle.
When adjusting the dosage of stimulants, women should be sure to keep a detailed observation log to track cycle fluctuations and the medication’s effects. This is the only way to determine whether the medication dosage needs to be adjusted during certain phases of the cycle. The dosage adjustment guide, available in the download section of adhd-forum.adxs.org , makes it easier to track medication intake, symptom progression, and the menstrual cycle.
11. Liver function
11.1. Age
Hepatic metabolism may slow down with age, due in part to reduced blood flow to the liver.289
Reduced CYP metabolism in older adults is known to occur with the following psychotropic drugs:2930
- Alprazolam (men only)
- Chlordiazepoxide
- Desipramine (men only)
- Diazepam
- Imipramine
- Nortriptyline
- Trazodone
- Triazolam (men only)
The rate of breakdown decreases by an average of 30 to 40 percent; however, this varies so much from person to person that, as with dosage determination, each case must be considered individually.
11.2. Diseases
Liver diseases can (significantly) impair liver function. Reduced protein synthesis in the liver automatically decreases plasma protein binding, which impairs the breakdown of substances by enzymes in the liver.
When bile production in the liver is impaired, the excretion of large molecules is reduced and the enterohepatic circulation is disrupted.
Heart failure reduces blood flow to the liver.
11.3. First-pass effect
“The intestinal veins carry blood to the heart via the liver, so that a substance absorbed in the intestine undergoes first-pass metabolism in the liver before it can be distributed further via the superior vena cava and the heart. If a substance survives this first-pass metabolism only to a small extent, this is referred to as a high first-pass effect. The result of this effect is that, despite good absorption, only small amounts of the active ingredient are available systemically. Due to the “first-pass effect,” substances can be rapidly metabolized or inactivated in the liver (presystemic elimination).”34
The first-pass effect also varies from person to person.
Starting at age 40, the first-pass effect decreases by about 1% each year, so that serum levels are higher in older adults when given the same dose.2930
11.4. Smoking
Smoking can affect metabolism by liver enzymes.
12. Receptor Sensitivity
Active pharmaceutical ingredients can bind to receptors, transporters, ion channels, or enzymes and trigger effects there. The sensitivity of these receptor structures influences the drug’s efficacy.
The sensitivity of the receptor structures can be influenced by variants in the genes that encode them.
Examples:
- A combination of six polymorphisms in genes encoding the 5-HT2A, 5-HT2C, and histamine H2 receptors, as well as SERT, predicted a response to clozapine in schizophrenia with a probability of just under 80%90
- Lack of efficacy of tamoxifen in breast cancer in the absence of estrogen receptor expression91
- Regarding ADHD medications, the influence of the DAT gene on the response to MPH is discussed
- Even when blood levels of vitamin D3 are sufficient, receptors with reduced sensitivity can still lead to a vitamin D3 deficiency
13. Blood-Brain Barrier: Passage into the Brain
The blood-brain barrier tightly seals off blood vessels in the brain to prevent uncontrolled exchange of substances into the brain. Ideally, only a controlled exchange via transporters and vesicles should take place.
The blood-brain barrier comprises a series of physiological properties that must either be induced (tight junctions, transporters, metabolic enzymes) or inhibited (transcytosis, LAM) in the brain’s endothelial cells compared to those in the rest of the body.92
A basic introduction to the blood-brain barrier in German can be found at Psysiologie.cc93; in English, see Daneman and Prat.92
Example:
- P-glycoprotein (MDR1 gene): controls the transport of drugs into the brain
- MDR1 gene variants influence its effectiveness. Reduced MDR1 function weakens the blood-brain barrier, allowing drugs to cross into the brain in greater quantities, which can increase their effect even though the blood plasma level remains unchanged.91
Imbalances in the gut microbiome can affect the blood-brain barrier, thereby impairing the brain’s protection against toxins and pathogens or its supply of nutrients. For more on this, see Gut-Brain Axis and ADHD in the chapter “ : Pathogenesis”
Learn more about the blood-brain barrier at Blood-Brain Barrier and ADHD In the chapter “ : Causes”
14. Metabolic enzymes: Degradation
Many drugs are broken down by enzymes, primarily in the liver.
Some active ingredients are formed only after a prior enzymatic conversion of the drug substances.
Effect strength: Depending on the gene variant, the enzyme encoded by the gene is synthesized in greater or lesser amounts, which affects its degradation capacity.
Competition: When multiple medications that are metabolized by the same enzyme are taken, they compete for that enzyme, which prolongs the duration of action of these medications and increases the risk of side effects.
In addition, there are active ingredients that inhibit (inhibitors) or promote (inducers) an enzyme, which accordingly affects their effectiveness in terms of drug metabolism.
In humans, metabolic enzymes catalyze two types of biotransformation reactions91
- Phase 1 reactions:
- Functionalization reactions
- Oxidation, reduction, hydrolysis, and hydration
- Mechanism of action:
- Introduction of a functional group (or groups) (e.g., a hydroxyl group) into the nonpolar molecule, or
- Identification of relevant functional groups
- Functionalization reactions
- Phase 2 reactions
- Conjugation reactions
- glucuronidation, sulfation, methylation, acetylation, and conjugation with amino acids and glutathione
- Mechanism of action:
- Binding of functional groups to highly polar, negatively charged endogenous molecules (e.g., glucuronic acid)
- Conjugation reactions
In the following, we will focus only on the enzymes that are relevant to ADHD medications. However, this already covers the most important enzymes.
CYP3A4 (guanfacine) metabolizes 40 to 50% of all medications.
CYP2D6 (amphetamine-based medications, atomoxetine) metabolizes about 25% of all medications.
14.1. Metabolism increases or decreases depending on the metabolic enzyme gene variant
The breakdown of active ingredients or neurotransmitters is influenced by how active the gene variant is that expresses the protein responsible for synthesizing their metabolic enzymes. Some gene variants result in increased or excessive protein production, while others result in reduced or no protein production at all.
In individuals with the COMT Val-158-Met gene polymorphism, amphetamine increases PFC efficiency in subjects with presumably low dopamine levels in the PFC. In contrast, in individuals with the COMT Met-158-Met polymorphism, amphetamine had no effect on cortical efficiency under low- to moderate-level working memory load and caused a decline under high-level working memory load. Individuals with the Met-158-Met polymorphism appear to have an increased risk of an adverse reaction to amphetamine.94
14.1.1. ADHD Active Ingredients and Their Primary Metabolizing Enzymes
ADHD active ingredients are broken down by various enzymes:
Methylphenidate: CES1
Amphetamine-based medications: CYP2D6 (also highly dependent on pH)
Atomoxetine: CYP2D6
Bupropion: CYP2B691 and a bit about CYP2A6
Guanfacine: CYP3A4
Clonidine: unknown
Buspirone: CYP3A4
Memantine: unknown; likely not metabolized by CYP44
Viloxazine: CYP2D6, UGT1A9, UGT2B15, and possibly also CYP1A2
Melatonin: CYP1A
Dasotralin: unknown
Agomelatine: CYP1A2 (90%), CYP2C9/2C19 (10%)
See the comprehensive articles on the metabolic enzymes associated with the respective ADHD medications:
- Methylphenidate (MPH)
- Amphetamine-based medications (AMP)
- Atomoxetine
- Bupropion: CYP2B6-91, and to a lesser extent CYP2A6; however, it is a strong CYP2D6 inhibitor
- Guanfacine
- Buspirone
14.1.2. Pharmacogenetic Diagnostics
Genetic testing can be used to identify genetic variants of metabolic enzymes.95
You can find suitable laboratories by searching for “Laboratory CES1” (for MPH) or “Laboratory CYP2D6” (amphetamine medications, atomoxetine). In Germany, the cost of this laboratory service should be covered by health insurance if it has been prescribed by a doctor.
As of September 2023, a laboratory test for the 22 most important metabolism-related genes (including the POR gene, which is important for the CYP gene family) cost approximately 600 €.
A sample diagnostic report is available from CeGaT, a provider of genetic diagnostics in Tübingen.96 Genetic analyses of individual metabolism-related genes cost around 300 € in September 2023.
14.2. Competition for Depletion and Cross-Effects
The effects of medications can be influenced in various ways by the enzymes that break them down.
Risk:
The mechanisms of competition, inhibition, induction, or modulation of gene expression described below must be taken into account when planning medication regimens. Failure to do so poses a risk or may even constitute medical malpractice. A new medication can affect the effect of a medication already being administered (and vice versa), thereby creating a risk of reduced efficacy and/or overdose of the new medication or the existing medication(s).
Benefits:
However, these same mechanisms of action can also be harnessed intentionally and prove beneficial.
Conversely, a deliberate combination of drugs that compete with, inhibit, or genetically regulate one another can be helpful in enhancing the effectiveness of individual drugs. Thus, when drugs are administered simultaneously, their dosages can be adjusted—either more cautiously or more aggressively—depending on the interactions involved. Similarly, such combinations can be used strategically, for example, to enhance the effect in ultra-rapid metabolizers or to improve drug clearance in slow metabolizers.
Example: A person with ADHD who metabolized a dose of Vyvanse in 5–6 hours, , reported to us that combining it with 150 mg of bupropion was very helpful in prolonging the duration of action of Vyvanse. Vyvanse is metabolized via CYP2D6; bupropion genetically inhibits CYP2D6.
14.2.1. Competition
Competition with other substrates: When multiple active ingredients bind to the same enzyme (substrates) and are broken down by it, they compete for the available amount of degrading enzymes when administered simultaneously. This can delay degradation.
14.2.2. Inhibition
Inhibition: Drugs can interfere with (inhibit) the action of enzymes, even if they are broken down by entirely different enzymes
14.2.3. Induction
Induction: Drugs can enhance (induce) the action of enzymes
14.2.4. Genetic Regulation
Genetic Regulation: Drug active ingredients can also influence metabolic enzymes through genetic regulation.
For example, in vitro, bupropion is only a relatively weak inhibitor of CYP2D6. In vivo, however, bupropion strongly inhibits CYP2D6 because it also causes genetic downregulation of CYP2D6 mRNA.97
15. Excretion: Renal Blood Flow
Since amphetamine is excreted by the kidneys, renal blood flow—in addition to the total dose—plays a small but measurable role in the duration of action.5
Another consequence of this is that blood levels of amphetamine change more slowly and are less prone to rebound than with methylphenidate,5
The glomerular filtration rate decreases on average by 8 ml/min/1.73 m² per decade (0.1 ml/s/m² per decade) starting at age 40. There are significant individual differences.
Serum creatinine levels often remain within the normal range in older adults despite a decrease in glomerular filtration rate, due to reduced muscle mass and decreased physical activity; as a result, serum creatinine levels no longer reflect normal kidney function in older adults. The clearance of psychotropic drugs excreted by the kidneys is reduced in older adults:2930
- Brexpiprazole
- Lurasidone
- Paliperidone
- Risperidone
16. Gene Variants and Response
A GWAS identified the effects of various genes on the response to MPH and ATX:98
- on chromosome 12, SNP: rs10880574, in the 5’-prime UTR-intron region of the TMEM117 gene (transmembrane protein 117). TMEM117 is located in the plasma membrane and is also involved in the intrinsic apoptotic signaling pathway in response to stress in the endoplasmic reticulum.
- on chromosome 18, SNP: rs2000900. Nearest gene: MYO5B (myosin 5B), which is involved in vesicular transport and, in a complex with RAB11A and RAB11FIP2, is required for the transport of NPC1L1 to the plasma membrane. MYO5B is primarily expressed in digestive organs and plays a role in metabolic processes.
- NKAIN2, a candidate gene for ADHD
- PUS7L
- CTD-2561J22.3.
Weih, Haen (2023): Therapeutisches Drug Monitoring in der Psychiatrie; NeuroTransmitter 2023; 34 (7-8), S. 25 - 29; deutsch ↥ ↥
Le (2022): Übersicht Pharmakokinetik; MSD manuals deutsch ↥ ↥
Le (2022): Übersicht Pharmakokinetik; MSD manuals englisch ↥
Rodden (2021): Short-Acting Stimulants Vs. Long-Acting Stimulants: Comparing ADHD Medications and Durations; Stand 14.09.2022 ↥ ↥
Dodson WW (2005): Pharmacotherapy of adult ADHD. J Clin Psychol. 2005 May;61(5):589-606. doi: 10.1002/jclp.20122. PMID: 15723384. REVIEW ↥ ↥ ↥ ↥
Umfrage ADxS.org, n = 23; Stand 09.09.23 ↥
Elbe, Black, McGrane, Procyshyn (Hrsg.) (2019): Clinical Handbook of Psychotrophic Drugs for Children and Adolescents, 4th edition ↥ ↥ ↥ ↥
https://www.kinderaerzte-im-netz.de/media/53ec94e833af614b730097d1/source/20080530092715_adhs2.pdf ↥ ↥ ↥ ↥
Umfrage ADxS.org, n = 100; Stand 09.09.23 ↥
Umfrage ADxS.org, n = 20; Stand 09.09.23 ↥
Rodden (2021): Short-Acting Stimulants Vs. Long-Acting Stimulants: Comparing ADHD Medications and Durations; Stand14.09.2022 ↥
Umfrage ADxS.org, n = 15; Stand 09.09.23 ↥
Medikamenten-Fachinformation des Herstellers ratiopharm ↥
Fachinformation Gelbe Liste Methylphenidathydrochlorid Hexal ↥
Kohns (2019): Arzneimittel in der Therapie der Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung (ADHS), neue Akzente 3/19 ↥
Dolder PC, Strajhar P, Vizeli P, Hammann F, Odermatt A, Liechti ME (2017): Pharmacokinetics and Pharmacodynamics of Lisdexamfetamine Compared with D-Amphetamine in Healthy Subjects. Front Pharmacol. 2017 Sep 7;8:617. doi: 10.3389/fphar.2017.00617. PMID: 28936175; PMCID: PMC5594082. ↥
Kämmerer W (2024): Comparative pharmacology and abuse potential of oral dexamphetamine and lisdexamfetamine-A literature review. Hum Psychopharmacol. 2024 Jul 18:e2910. doi: 10.1002/hup.2910. PMID: 39024047. REVIEW ↥ ↥
Childress AC, Findling RL, Wu J, Kollins SH, Wang Y, Martin P, Robertson B (2020): Lisdexamfetamine Dimesylate for Preschool Children with Attention-Deficit/Hyperactivity Disorder. J Child Adolesc Psychopharmacol. 2020 Apr;30(3):128-136. doi: 10.1089/cap.2019.0117. PMID: 32233956; PMCID: PMC7153646. ↥
Adler LA, Alperin S, Leon T, Faraone SV (2017): Pharmacokinetic and Pharmacodynamic Properties of Lisdexamfetamine in Adults with Attention-Deficit/Hyperactivity Disorder. J Child Adolesc Psychopharmacol. 2017 Mar;27(2):196-199. doi: 10.1089/cap.2016.0121. PMID: 27935735. ↥
Ermer J, Corcoran M, Lasseter K, Marbury T, Yan B, Martin PT (2016): A Single-Dose, Open-Label Study of the Pharmacokinetics, Safety, and Tolerability of Lisdexamfetamine Dimesylate in Individuals With Normal and Impaired Renal Function. Ther Drug Monit. 2016 Aug;38(4):546-55. doi: 10.1097/FTD.0000000000000296. PMID: 26926668; PMCID: PMC4949011. ↥
Boellner SW, Stark JG, Krishnan S, Zhang Y (2010): Pharmacokinetics of lisdexamfetamine dimesylate and its active metabolite, d-amphetamine, with increasing oral doses of lisdexamfetamine dimesylate in children with attention-deficit/hyperactivity disorder: a single-dose, randomized, open-label, crossover study. Clin Ther. 2010 Feb;32(2):252-64. doi: 10.1016/j.clinthera.2010.02.011. PMID: 20206783. ↥
Ermer J, Homolka R, Martin P, Buckwalter M, Purkayastha J, Roesch B (2010): Lisdexamfetamine dimesylate: linear dose-proportionality, low intersubject and intrasubject variability, and safety in an open-label single-dose pharmacokinetic study in healthy adult volunteers. J Clin Pharmacol. 2010 Sep;50(9):1001-10. doi: 10.1177/0091270009357346. PMID: 20173084. ↥
Information Takeda, 24.04.2024 ↥
Hahn, Wolters (2001): Lebensmittel-Medikamenten-Interaktionen. in: LEXIKON DER ERNÄHRUNG. Spektrum.de. Abgerufen 28.01.23 ↥
Ruscin, Linnebur (2021): Pharmakokinetik bei Älteren; MSD manuals deutsch ↥ ↥ ↥ ↥ ↥
Ruscin, Linnebur (2021): Pharmacokinetics in Older Adults; MSD manuals englisch ↥ ↥ ↥ ↥ ↥
Krabseth HM, Strømmen M, Helland A, Spigset O (2025): Effect of bariatric surgery on the pharmacokinetics of drugs used for attention-deficit hyperactivity disorder-A case series. Basic Clin Pharmacol Toxicol. 2025 Jan;136(1):e14099. doi: 10.1111/bcpt.14099. PMID: 39497274; PMCID: PMC11655785. ↥
Jones (2022): Pharmakokinetik bei Kindern, MDS manuals deutsch ↥
Jones (2022): Pharmacokinetics in Children, MDS manuals englisch ↥
WikiBooks: Pharmakologie und Toxikologie: Pharmakokinetik, 26.01.2023 ↥ ↥
Wisker (2010): Interaktionen zwischen Nahrung und Arzneimitteln; Ernährungs Umschau | 3/10 ↥ ↥
ELLIOT JS, SHARP RF, LEWIS L (1959): Urinary pH. J Urol. 1959 Feb;81(2):339-43. doi: 10.1016/S0022-5347(17)66022-1. PMID: 13631832. ↥ ↥ ↥ ↥ ↥ ↥
BECKETT AH, ROWLAND M, TURNER P (1965): INFLUENCE OF URINARY PH ON EXCRETION OF AMPHETAMINE. Lancet. 1965 Feb 6;1(7380):303. doi: 10.1016/s0140-6736(65)91033-0. PMID: 14247879. ↥ ↥ ↥ ↥
Kim I, Oyler JM, Moolchan ET, Cone EJ, Huestis MA (2004): Urinary pharmacokinetics of methamphetamine and its metabolite, amphetamine following controlled oral administration to humans. Ther Drug Monit. 2004 Dec;26(6):664-72. doi: 10.1097/00007691-200412000-00013. PMID: 15570192. ↥
Clarke, E. G. C. (Ed.). (1969). Isolation and identification of drugs (Vol. 1, pp. 192-193). London: Pharmaceutical press. ↥
Tekada Fachinformation Elvanse abgerufen 04.02.23 ↥ ↥
Chan C, Sui W, Breeggemann MC, Stoller M (2025): Modulators of urinary pH in the context of urinary stone disease: a literature review. Transl Androl Urol. 2025 Aug 30;14(8):2428-2438. doi: 10.21037/tau-2025-275. Epub 2025 Aug 26. PMID: 40949433; PMCID: PMC12433178. REVIEW ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥
Osuna-Padilla IA, Leal-Escobar G, Garza-García CA, Rodríguez-Castellanos FE (2019): Dietary Acid Load: mechanisms and evidence of its health repercussions. Nefrologia (Engl Ed). 2019 Jul-Aug;39(4):343-354. English, Spanish. doi: 10.1016/j.nefro.2018.10.005. PMID: 30737117. REVIEW ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥
Memantine Merz, ANHANG I, ZUSAMMENFASSUNG DER MERKMALE DES ARZNEIMITTELS ↥ ↥ ↥ ↥
Huang W, Czuba LC, Isoherranen N (2020): Mechanistic PBPK Modeling of Urine pH Effect on Renal and Systemic Disposition of Methamphetamine and Amphetamine. J Pharmacol Exp Ther. 2020 Jun;373(3):488-501. doi: 10.1124/jpet.120.264994. PMID: 32198137; PMCID: PMC7250368. ↥ ↥
Aresti-Sanz J, Schwalbe M, Pereira RR, Permentier H, El Aidy S (2021): Stability of Methylphenidate under Various pH Conditions in the Presence or Absence of Gut Microbiota. Pharmaceuticals (Basel). 2021 Jul 27;14(8):733. doi: 10.3390/ph14080733. PMID: 34451830; PMCID: PMC8398889. ↥ ↥ ↥
Yang X, Morris SM, Gearhart JM, Ruark CD, Paule MG, Slikker W Jr, Mattison DR, Vitiello B, Twaddle NC, Doerge DR, Young JF, Fisher JW (2014): Development of a physiologically based model to describe the pharmacokinetics of methylphenidate in juvenile and adult humans and nonhuman primates. PLoS One. 2014 Sep 3;9(9):e106101. doi: 10.1371/journal.pone.0106101. PMID: 25184666; PMCID: PMC4153582. ↥ ↥
Yang X, Duan J, Fisher J (2016): Application of Physiologically Based Absorption Modeling to Characterize the Pharmacokinetic Profiles of Oral Extended Release Methylphenidate Products in Adults. PLoS One. 2016 Oct 10;11(10):e0164641. doi: 10.1371/journal.pone.0164641. PMID: 27723791; PMCID: PMC5056674. ↥
Sui W, Miller NL, Gould ER, Zhang KC, Koyama T, Hsi RS (2022): Proton pump inhibitors use and risk of incident nephrolithiasis. Urolithiasis. 2022 Aug;50(4):401-409. doi: 10.1007/s00240-022-01326-1. PMID: 35499617. ↥ ↥
Zieglmaier (2014): Methylphenidat bei Erwachsenen. Was ist bei der Therapie zu beachten? DAZ.ONLINE DAZ / AZ DAZ 44/2014 ↥
Cook JD, Strauss KA, Caplan YH, Lodico CP, Bush DM (2007): Urine pH: the effects of time and temperature after collection. J Anal Toxicol. 2007 Oct;31(8):486-96. doi: 10.1093/jat/31.8.486. PMID: 17988463. ↥ ↥ ↥
Alguacil J, Kogevinas M, Silverman DT, Malats N, Real FX, García-Closas M, Tardón A, Rivas M, Torà M, García-Closas R, Serra C, Carrato A, Pfeiffer RM, Fortuny J, Samanic C, Rothman N (2011): Urinary pH, cigarette smoking and bladder cancer risk. Carcinogenesis. 2011 Jun;32(6):843-7. doi: 10.1093/carcin/bgr048. PMID: 21402590; PMCID: PMC3106435. ↥
Guiol C, Montastruc P, Prévost MC (1986): Renal effect of acute hypobaric pressure breathing in normal and diabetes insipidus rats. J Physiol (Paris). 1986;81(1):41-4. PMID: 3761205. ↥
Beara-Lasic L, Goldfarb DS (2020): Nephrolithiasis in women: how different from men? Curr Opin Nephrol Hypertens. 2020 Mar;29(2):201-206. doi: 10.1097/MNH.0000000000000577. PMID: 31789849. REVIEW ↥ ↥
Menezes CJ, Worcester EM, Coe FL, Asplin J, Bergsland KJ, Ko B (2019): Mechanisms for falling urine pH with age in stone formers. Am J Physiol Renal Physiol. 2019 Jul 1;317(7):F65-F72. doi: 10.1152/ajprenal.00066.2019. PMID: 31017011; PMCID: PMC6692718. ↥ ↥ ↥
Otto BJ, Bozorgmehri S, Kuo J, Canales M, Bird VG, Canales B (2017): Age, Body Mass Index, and Gender Predict 24-Hour Urine Parameters in Recurrent Idiopathic Calcium Oxalate Stone Formers. J Endourol. 2017 Dec;31(12):1335-1341. doi: 10.1089/end.2017.0352. PMID: 29084490. ↥ ↥
Taylor GO, Oyediran AB, Adesina HA (1979): The effect of seasonal changes and socio-economic status on urinary pH and specific gravity. Trop Geogr Med. 1979 Mar;31(1):105-10. PMID: 39374. ↥ ↥
Zechner O, Latal D, Pflüger H, Scheiber V (1981): Die soziale Infrastruktur von Harnsteinpatienten [The social infrastructure of patients with urinary calculi (author’s transl)]. Wien Klin Wochenschr. 1981 Oct 30;93(20):635-8. German. PMID: 7324475. ↥ ↥
Barclay H, Mukerji S, Kayser B, O’Donnell T, Tzeng YC, Hill S, Knapp K, Legg S, Frei D, Fan JL (2021): Respiratory alkalinization and posterior cerebral artery dilatation predict acute mountain sickness severity during 10 h normobaric hypoxia. Exp Physiol. 2021 Jan;106(1):175-190. doi: 10.1113/EP088938. PMID: 33347666. ↥
Kass MA, Kolker AE, Gordon M, Goldberg I, Gieser DK, Krupin T, Becker B (1981): Acetazolamide and urolithiasis. Ophthalmology. 1981 Mar;88(3):261-5. doi: 10.1016/s0161-6420(81)35041-6. PMID: 7231915. ↥
Drewa T, Wolski Z, Gruszka M, Misterek B, Lysik J (2007): Uric acid plasma level and urine pH in rats treated with ambroxol. Acta Pol Pharm. 2007 Nov-Dec;64(6):565-7. PMID: 18323253. ↥
Nazzal L, Francois F, Henderson N, Liu M, Li H, Koh H, Wang C, Gao Z, Perez GP, Asplin JR, Goldfarb DS, Blaser MJ (2021): Effect of antibiotic treatment on Oxalobacter formigenes colonization of the gut microbiome and urinary oxalate excretion. Sci Rep. 2021 Aug 12;11(1):16428. doi: 10.1038/s41598-021-95992-7. PMID: 34385560; PMCID: PMC8361114. ↥
Siener R (2016): Can the manipulation of urinary pH by beverages assist with the prevention of stone recurrence? Urolithiasis. 2016 Feb;44(1):51-6. doi: 10.1007/s00240-015-0844-7. PMID: 26614113. REVIEW ↥ ↥
Biolo G, Di Girolamo FG, Heer M, Sturma M, Mazzucco S, Agostini F, Situlin R, Vinci P, Giordano M, Buehlmeier J, Frings-Meuthen P, Mearelli F, Fiotti N (2019): Alkalinization with potassium bicarbonate improves glutathione status and protein kinetics in young volunteers during 21-day bed rest. Clin Nutr. 2019 Apr;38(2):652-659. doi: 10.1016/j.clnu.2018.04.006. PMID: 29739680. ↥
Cao C, Li F, Ding Q, Jin X, Tu W, Zhu H, Sun M, Zhu J, Yang D, Fan B (2024): Potassium sodium hydrogen citrate intervention on gut microbiota and clinical features in uric acid stone patients. Appl Microbiol Biotechnol. 2024 Dec;108(1):51. doi: 10.1007/s00253-023-12953-y. PMID: 38183479; PMCID: PMC10771603. ↥
Classen HG, Fischer G, Marx J, Schimatschek H, Schmid C, Stein C (1987): Prevention of stress-induced damage in experimental animals and livestock by monomagnesium-L-aspartate hydrochloride. Magnesium. 1987;6(1):34-9. PMID: 3821173. ↥ ↥
Nahok K, Phetcharaburanin J, Li JV, Silsirivanit A, Thanan R, Boonnate P, Joonhuathon J, Sharma A, Anutrakulchai S, Selmi C, Cha’on U (2021): Monosodium Glutamate Induces Changes in Hepatic and Renal Metabolic Profiles and Gut Microbiome of Wistar Rats. Nutrients. 2021 May 30;13(6):1865. doi: 10.3390/nu13061865. PMID: 34070818; PMCID: PMC8229789. ↥
Fukushima S, Uwagawa S, Shirai T, Hasegawa R, Ogawa K (1990): Synergism by sodium L-ascorbate but inhibition by L-ascorbic acid for sodium saccharin promotion of rat two-stage bladder carcinogenesis. Cancer Res. 1990 Jul 15;50(14):4195-8. PMID: 2364375. ↥
Baia Lda C, Baxmann AC, Moreira SR, Holmes RP, Heilberg IP (2012): Noncitrus alkaline fruit: a dietary alternative for the treatment of hypocitraturic stone formers. J Endourol. 2012 Sep;26(9):1221-6. doi: 10.1089/end.2012.0092. PMID: 22500592. ↥
Ghorbe F, Boujelbene M, Makni-Ayadi F, Guermazi F, Kammoun A, Murat J, Croute F, Soleilhavoup JP, El-Feki A (2001): Effect of chronic lead exposure on kidney function in male and female rats: determination of a lead exposure biomarker. Arch Physiol Biochem. 2001 Dec;109(5):457-63. doi: 10.1076/apab.109.5.457.8035. PMID: 11935388. ↥
Schneider SN, Liu Z, Wang B, Miller ML, Afton SE, Soleimani M, Nebert DW (2014): Oral cadmium in mice carrying 5 versus 2 copies of the Slc39a8 gene: comparison of uptake, distribution, metal content, and toxicity. Int J Toxicol. 2014 Jan-Feb;33(1):14-20. doi: 10.1177/1091581813513530. PMID: 24345748. ↥
Arphorn S, Manothum A, Santiwung K, Pangunta K, Hara K, Ishimaru T (2021): Working Conditions and Urinalysis Dipstick Testing among Female Rice Farmers: A Preliminary Cross-Sectional Study. Int J Environ Res Public Health. 2021 Aug 25;18(17):8942. doi: 10.3390/ijerph18178942. PMID: 34501531; PMCID: PMC8430999. ↥
García-Trabanino R, Jarquín E, Wesseling C, Johnson RJ, González-Quiroz M, Weiss I, Glaser J, José Vindell J, Stockfelt L, Roncal C, Harra T, Barregard L (2015): Heat stress, dehydration, and kidney function in sugarcane cutters in El Salvador–A cross-shift study of workers at risk of Mesoamerican nephropathy. Environ Res. 2015 Oct;142:746-55. doi: 10.1016/j.envres.2015.07.007. PMID: 26209462. ↥
Wesseling C, Aragón A, González M, Weiss I, Glaser J, Rivard CJ, Roncal-Jiménez C, Correa-Rotter R, Johnson RJ (2016): Heat stress, hydration and uric acid: a cross-sectional study in workers of three occupations in a hotspot of Mesoamerican nephropathy in Nicaragua. BMJ Open. 2016 Dec 8;6(12):e011034. doi: 10.1136/bmjopen-2016-011034. Erratum in: BMJ Open. 2017 Jan 25;7(1):e011034corr1. doi: 10.1136/bmjopen-2016-011034corr1. PMID: 27932336; PMCID: PMC5168614. ↥
Masterson JH, Jourdain VJ, Collard DA, Choe CH, Christman MS, L’Esperance JO, Auge BK (2013): Changes in urine parameters after desert exposure: assessment of stone risk in United States Marines transiently exposed to a desert environment. J Urol. 2013 Jan;189(1):165-70. doi: 10.1016/j.juro.2012.08.097. PMID: 23174258. ↥
Lee J, Chang HK, Lee S (2020): Association of low urine pH as a metabolic feature with abdominal obesity. J Int Med Res. 2020 Jan;48(1):300060519898615. doi: 10.1177/0300060519898615. PMID: 31992101; PMCID: PMC7113708. ↥
Fellström B, Danielson BG, Karlström B, Lithell H, Ljunghall S, Vessby B, Wide L (1984): Effects of high intake of dietary animal protein on mineral metabolism and urinary supersaturation of calcium oxalate in renal stone formers. Br J Urol. 1984 Jun;56(3):263-9. doi: 10.1111/j.1464-410x.1984.tb05384.x. PMID: 6544608. ↥
Cosgrove K, Johnston CS (2017): Examining the Impact of Adherence to a Vegan Diet on Acid-Base Balance in Healthy Adults. Plant Foods Hum Nutr. 2017 Sep;72(3):308-313. doi: 10.1007/s11130-017-0620-7. PMID: 28677099. ↥
Passey C (2017): Reducing the Dietary Acid Load: How a More Alkaline Diet Benefits Patients With Chronic Kidney Disease. J Ren Nutr. 2017 May;27(3):151-160. doi: 10.1053/j.jrn.2016.11.006. PMID: 28117137 REVIEW ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥
Vormann (2021): Ausführliche PRAL-Tabelle zu Wunderwaffe Basenfood ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥
Remer T, Manz F (1995): Potential renal acid load of foods and its influence on urine pH. J Am Diet Assoc. 1995 Jul;95(7):791-7. doi: 10.1016/S0002-8223(95)00219-7. PMID: 7797810. ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥ ↥
Passey C (2017): Reducing the Dietary Acid Load: How a More Alkaline Diet Benefits Patients With Chronic Kidney Disease. J Ren Nutr. 2017 May;27(3):151-160. doi: 10.1053/j.jrn.2016.11.006. PMID: 28117137 REVIEW ↥ ↥ ↥
https://adhs-forum.adxs.org/t/medi-wirkdauer-bei-sport/11700 ↥
Schoretsanitis, de Leon, Eap, Kane, Paulzen (2019): Clinically Significant Drug-Drug Interactions with Agents for Attention-Deficit/Hyperactivity Disorder. CNS Drugs. 2019 Dec;33(12):1201-1222. doi: 10.1007/s40263-019-00683-7. ↥
Le (2022): Overview of Pharmacokinetics; MSD manuals englisch ↥
Arranz MJ, Collier D, Kerwin RW (2001): Pharmacogenetics for the individualization of psychiatric treatment. Am J Pharmacogenomics. 2001;1(1):3-10. doi: 10.2165/00129785-200101010-00001. PMID: 12173312. ↥
Schwab, Matthias; Marx, Claudia; Zanger, Ulrich M.; Eichelbaum, Michel; Fischer-Bosch, Margarete (2002): Pharmakogenetik der Zytochrom-P-450-Enzyme: Bedeutung für Wirkungen und Nebenwirkungen von Medikamenten. Dtsch Arztebl 2002; 99(8): A-497 / B-400 / C-377 ↥ ↥ ↥ ↥ ↥
Daneman R, Prat A (2015): The blood-brain barrier. Cold Spring Harb Perspect Biol. 2015 Jan 5;7(1):a020412. doi: 10.1101/cshperspect.a020412. PMID: 25561720; PMCID: PMC4292164. REVIEW ↥ ↥
Mattay, Goldberg, Fera, Hariri, Tessitore, Egan, Kolachana, Callicott, Weinberger (2003): Catechol O-methyltransferase val158-met genotype and individual variation in the brain response to amphetamine; doi: 10.1073/pnas.0931309100; PNAS May 13, 2003 vol. 100 no. 10 6186-6191 ↥
Kein, Grau (2001): Arzneimittelnebenwirkungen vermeiden: Möglichkeiten der pharmakogenetischen Diagnostik. J Lab Med 2001; 25 (11/12): 477-484 ↥
Sager JE, Tripathy S, Price LS, Nath A, Chang J, Stephenson-Famy A, Isoherranen N (2017): In vitro to in vivo extrapolation of the complex drug-drug interaction of bupropion and its metabolites with CYP2D6; simultaneous reversible inhibition and CYP2D6 downregulation. Biochem Pharmacol. 2017 Jan 1;123:85-96. doi: 10.1016/j.bcp.2016.11.007. Erratum in: Biochem Pharmacol. 2021 Jan;183:114306. PMID: 27836670; PMCID: PMC5164944. ↥
Zhao Y, Fu Z, Barnett EJ, Wang N, Zhang K, Gao X, Zheng X, Tian J, Zhang H, Ding X, Li S, Li S, Cao Q, Chang S, Wang Y, Faraone SV, Yang L (2025): Genome data based deep learning identified new genes predicting pharmacological treatment response of attention deficit hyperactivity disorder. Transl Psychiatry. 2025 Feb 7;15(1):46. doi: 10.1038/s41398-025-03250-5. PMID: 39920114; PMCID: PMC11806042. ↥